A brief guide for patients with cold agglutinin disease
For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Cold agglutinin disease (CAD) is a rare condition that affects red blood cells.
Many people live well with it for years.
Having CAD does not automatically mean a dangerous or life-threatening illness.
Doctors focus on symptoms, patterns, and changes over time to understand what it means for you personally.
First things first
Not all anemia is the same.
CAD is a specific type of anemia caused by the immune system reacting to red blood cells, especially in cooler temperatures. Understanding this pattern helps doctors choose the right tests, monitoring plan, and treatment approach.
What it is
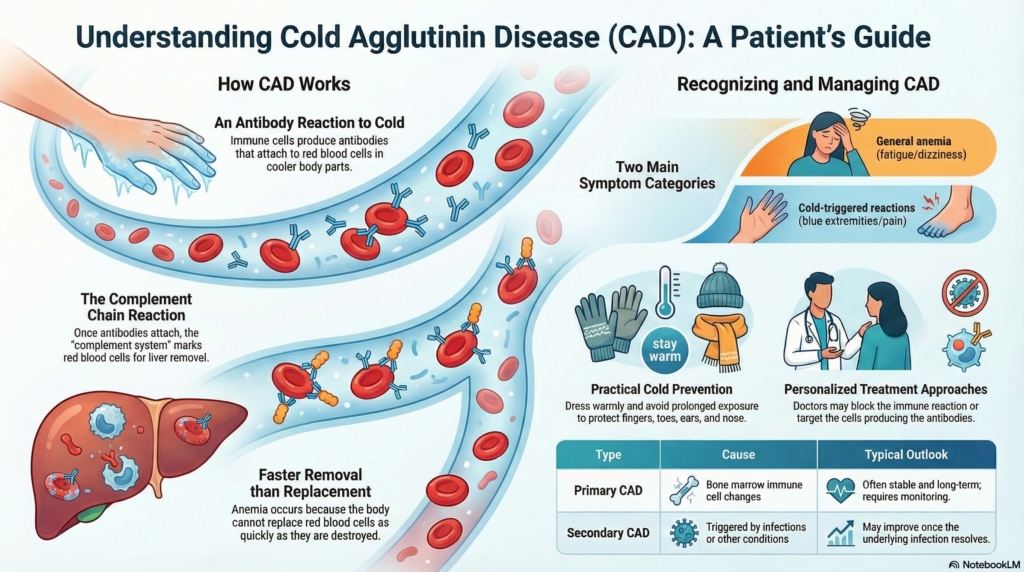
Cold agglutinin disease is a condition in which the immune system makes antibodies that attach to red blood cells, particularly when blood cools in areas like the fingers, toes, ears, or nose.
When these antibodies attach, they can trigger a natural immune reaction called complement activation, which marks red blood cells for removal. Over time, this can cause red blood cells to be destroyed faster than your body replaces them, leading to anemia.
You may see the word complement in lab reports or discussions. It simply refers to this immune reaction chain.
Why it happens (causes)
CAD occurs when a small group of immune cells produces these antibodies.
This may happen:
- on its own (called primary CAD)
- after certain infections
- alongside another immune or blood condition
In many adults with primary CAD, the antibody comes from a slow-growing group of immune cells in the bone marrow. This does not mean an aggressive cancer. Many people remain stable for years.
Most cases are not caused by anything a person did or could have prevented.
Does it cause symptoms?
Symptoms vary widely.
Some people have none. Others experience one or both of these symptom types:
Anemia-related symptoms
- fatigue
- shortness of breath
- pale or yellowish skin
- dark urine during episodes of increased red cell breakdown
Cold-triggered circulation symptoms
- fingers or toes turning pale or bluish
- numbness or tingling in cold environments
- discomfort in hands or feet
These two symptom groups can vary independently. Someone may have strong cold sensitivity but only mild anemia, or the opposite.
Symptoms may temporarily worsen during infections or cold weather.
Is it dangerous?
For most people, CAD is manageable and not immediately dangerous.
Doctors become more concerned when:
- anemia worsens
- symptoms interfere with daily life
- red blood cells are being destroyed rapidly
- hemoglobin drops significantly
Severe complications are uncommon. Many patients live for years with stable disease.
Why Cold Matters
Cold temperatures make the antibodies more likely to attach to red blood cells. This is why symptoms often appear in colder parts of the body.
Simple precautions can help:
- dressing warmly
- protecting hands and feet
- avoiding prolonged cold exposure
- warming IV fluids or blood transfusions if needed
These measures reduce symptoms and help prevent complications.
How your doctor evaluates it
Evaluation focuses on confirming the diagnosis and understanding how active the condition is.
Tests may include:
- blood counts to measure anemia
- markers of red blood cell breakdown
- tests that detect cold antibodies or complement activity
- evaluation for related conditions
A bone marrow biopsy is not needed for everyone. It is used only when doctors need more information about the antibody-producing cells or when results are unclear.
Testing is usually step-by-step rather than urgent unless symptoms are severe.
What is the treatment?
Treatment depends on symptoms, anemia severity, and how active the disease is.
Many people do not need treatment and are safely monitored over time. Observation means regular follow-up, not ignoring the condition.
When treatment is needed, there are two main approaches:
Control-focused therapy
These treatments block the immune reaction (complement) that damages red blood cells. They can improve anemia quickly but usually must be continued.
Cause-focused therapy
Other treatments target the immune cells making the antibody. These may take longer to work but can provide longer-lasting benefit.
Your doctor recommends treatment based on symptoms, lab patterns, speed of change, and your preferences.
Daily life and self-care
Most people with CAD can continue their usual activities.
Helpful habits:
- staying warm in cold environments
- avoiding sudden temperature changes
- treating infections promptly
- telling healthcare providers about CAD before procedures
- keeping follow-up appointments
Brief cold exposure, such as walking outside for a short time, is usually well tolerated.
When should I contact my doctor?
Let your healthcare team know if you notice:
- worsening fatigue
- shortness of breath at rest
- chest pain
- fainting or near-fainting
- persistent dark urine
- rapidly worsening symptoms
These signs may indicate more active anemia and should be evaluated.
What is the usual plan going forward?
Most people with CAD are monitored over time with periodic visits and blood tests.
Doctors focus on:
- stability versus change
- symptom burden
- trends in hemoglobin
Long periods of stability are common.
Making sense of it
CAD is best understood as a condition of context and thresholds, not constant danger. The immune system behaves differently at different temperatures, and the body often adapts well.
Knowing when the condition matters, and when it does not, helps prevent unnecessary worry and unnecessary treatment.
Key takeaways
- CAD is a condition where antibodies affect red blood cells, especially in the cold
- many people feel well and may not need treatment
- symptoms can involve anemia, cold-triggered changes, or both
- treatment decisions depend on symptoms and overall impact, not just lab numbers
- trends over time matter more than a single test result
For clinicians: Read our detailed guide on how to communicate about CAD to patients.