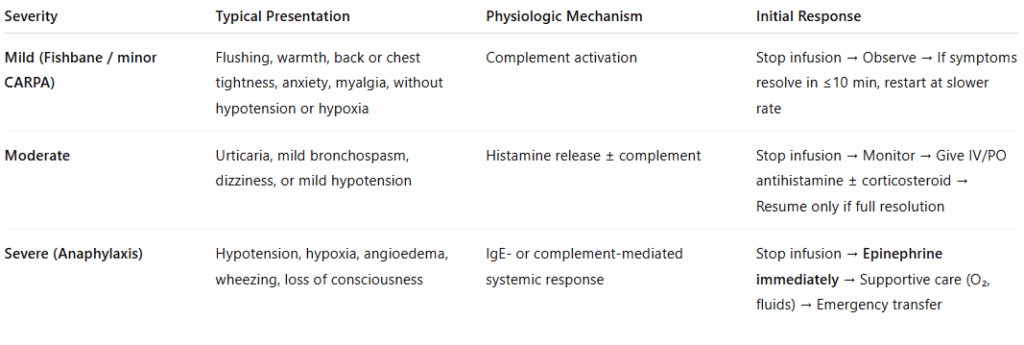
Mild (Fishbane / minor CARPA):
- Stop infusion → Observe → If symptoms resolve in ≤10 min, restart at slower rate
- Step-by-Step Management:
- Stop the infusion.
- Observe — symptoms typically resolve within 5–10 min.
- When completely resolved:
- Restart infusion at ≤50% rate.
- Monitor closely.
- If symptoms recur → stop and do not restart.
- Do not give premedication for future infusions; it’s not preventive and can mask early warning signs.
Moderate CARPA:
- Stop infusion → Monitor → Give IV/PO antihistamine ± corticosteroid → Resume only if full resolution
- Step-by-Step Management:
- Stop the infusion.
- Assess vitals; provide oxygen if needed.
- Administer:
- Diphenhydramine 25–50 mg IV or PO, or second-generation antihistamine if mild.
- Methylprednisolone 40–80 mg IV if persistent symptoms or recurrent reaction.
- Resume infusion only if symptoms completely resolve.
- Document event and consider switching formulation for future treatment.
Severe (Anaphylaxis):
- Stop infusion → Epinephrine immediately → Supportive care (O₂, fluids) → Emergency transfer
- Step-by-Step Management:
- Stop infusion immediately.
- Call for emergency assistance (code/EMS).
- Administer epinephrine promptly:
- 0.3–0.5 mg (0.3–0.5 mL of 1:1000) IM in mid-thigh; Repeat every 5–10 min if no improvement.
- Lay patient supine, elevate legs unless contraindicated.
- Oxygen 8–10 L/min via mask.
- IV fluids (normal saline or lactated Ringer’s) rapidly.
- Adjuncts:
- Antihistamine (diphenhydramine 25–50 mg IV)
- Corticosteroid (methylprednisolone 125 mg IV)
- Bronchodilator if wheezing (albuterol neb)
- Monitor continuously; prepare for airway management if needed.
- Transfer to emergency department for observation ≥4–6 h (risk of biphasic reaction).