What do the experts say?
- Teferi et al, 2025
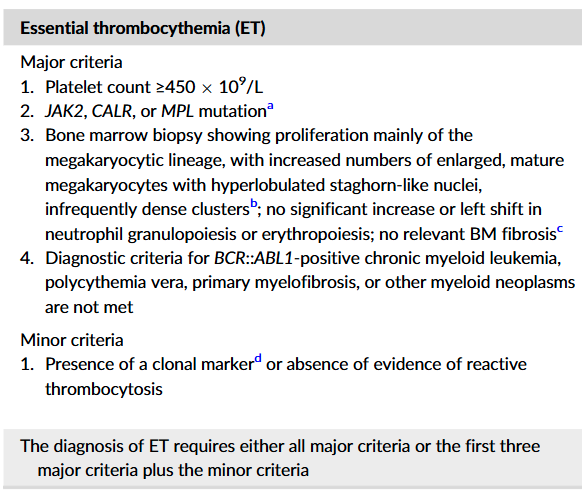
- Formal diagnostic criteria of essential thrombocythemia from the International Consensus Classification of Myeloid Neoplasms and Acute Leukemias and the World Health Organization:
- Includes 4 major criteria:
- Thrombocytosis (platelet count >450 × 109/L)
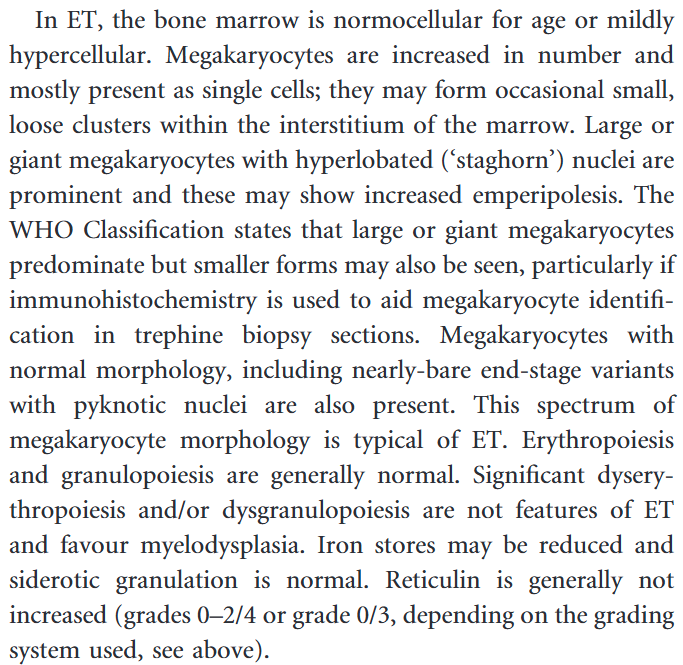
- Bone marrow examination that shows megakaryocyte proliferation of mature forms
- Exclusion of other myeloid neoplasms
- A driver variant in JAK2, CALR, and MPL.
- However, presence of the first 3 major criteria plus no evidence for secondary thrombocytosis is also sufficient to diagnose essential thrombocythemia.
- Godfrey et al, 2023
- The risk of post-ET myelofibrosis and thrombosis increases with age and in those with higher white blood cell counts, lower hemoglobin, and higher bone marrow reticulin grade at diagnosis.
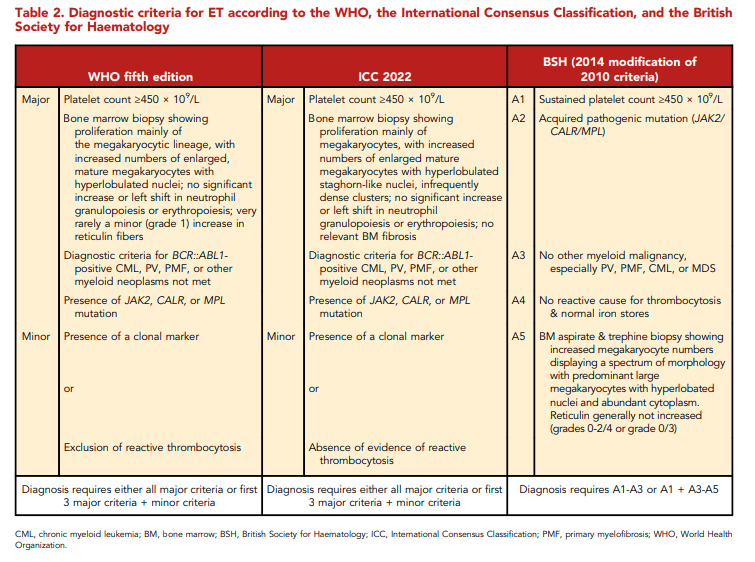
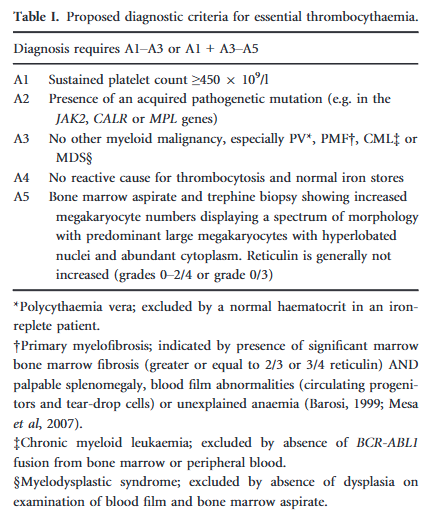
- Diagnostic criteria for ET according to the WHO, the International Consensus Classification, and the British Society for Haematology:
- Tefferi and Pardanani, 2019:
- “Confirmation of the diagnosis [of ET] requires a bone marrow biopsy”.
- “A bone marrow biopsy should be performed to distinguish essential thrombocythemia from its mimics, particularly prefibrotic myelofibrosis“.
- “Although a bone marrow biopsy is required for conclusive diagnosis, the presence of a driver mutation, combined with appropriate clinical features (e.g., normal levels of hemoglobin and serum lactate dehydrogenase and the absence of leukoerythroblastosis or dacryocytes), strongly suggests a diagnosis of essential thrombocythemia”.
- Mora and Passamontia, 2019
- “Bone marrow biopsy is essential for ET diagnosis and for distinguishing cases with prefibrotic PMF (pre-PMF) with an ET phenotype or PV with a lower level of hemoglobin”.
- While suspecting ET, it is standard practice to perform also bone marrow aspirate to rule out the presence of myelodysplasia (MDS) sideroblasts and thrombocytosis”.
- Advanced age, anemia, bone marrow hypercellularity, and increased reticulin fibers are considered risk factors for PET MF evolution.
- Gisslinger et al, 2017
- BCSH diagnostic criteria (A1-A3) allows ET diagnosis without BM morphology examination.
- Thus, BCSH does not allow of recognition of:
- Early/prefibrotic stages of PMF (prePMF):
- Only differentiates ET from overt PMF defined by significant BM fibrosis and palpable splenomegaly, blood film abnormalities (circulating progenitors and tear-drop cells) or unexplained anemia.
- This approach disregards early/prefibrotic stages of PMF (prePMF) associated with high platelet counts, which gets lumped into ET.
- Masked polycythemia vera:
- According to BCSH-criteria, PV is excluded by normal hematocrit levels in iron-replete patients.
- This may result in misdiagnosis of cases of masked PV in which the Hct is normal.
- Masked PV can be accurately diagnosed through BM biopsy.
- Early/prefibrotic stages of PMF (prePMF):
- “Thrombocythemic MPN are a heterogenic group of patients with different clinical and biological characteristics. However, without an exact differentiation, including BM biopsy examination, we never will be able to understand their potential differences in molecular genetic characteristics”.
What do the clinical guidelines say?
- NCCN Guidelines Version 1.202:
- Work up when suspicion of myeloproliferative neoplasms (MPN):
- Bone marrow aspirate with iron stain; bone marrow biopsy with trichrome and reticulin stain
- Bone marrow cytogenetics
- Molecular testing (blood or bone marrow)
- “Bone marrow aspirate with iron stain and biopsy with trichrome and reticulin stains and bone marrow cytogenetics (karyotype, with or without FISH; peripheral blood for FISH, if bone marrow is inaspirable) are necessary to accurately distinguish the bone marrow morphologic features between the disease subtypes (early or prefibrotic PMF, ET, and masked PV)”.
- Bone marrow aspirate and biopsy should be performed to rule out disease progression to MF prior to the initiation of cytoreductive therapy.
- In the 2017 WHO criteria, the diagnostic criteria for PV have been refined to differentiate masked PV from ET (recognizing the utility of bone marrow biopsy in patients with hemoglobin levels <18.5 g/dL in men and <16.5 g/dL in women).
- Work up when suspicion of myeloproliferative neoplasms (MPN):
- BSH, 2014:
- Bone marrow examination (aspirate and trephine biopsy) is required according to the WHO classification to make the diagnosis of ET.
- However, in elderly patients where a clonal marker, such as JAK2 V617F or MPL 515L/K has been detected, without features suspicious of MDS or primary myelofibrosis (PMF), a bone marrow examination may not be necessary.
- This represents a departure from the WHO classification.
- However the guidelines group agreed that this was justified for at least two reasons:
- Poor reproducibility in interpreting some trephine biopsy features
- The most recent WHO diagnostic criteria for all stages of PMF requires the presence of additional features such as splenomegaly, leucoerythroblastic film, or significant constitutional symptoms, that bone marrow examination was not always necessary.
- Nevertheless, it is recommended to perform a bone marrow biopsy where there are atypical features, or if during the course of treatment a change in management is planned, such as change of cytoreductive therapy, or if transformation is suspected. The guideline group therefore proposed a modification of the WHO diagnostic criteria for ET:
- The international consensus classification of myeloid neoplasms and acute Leukemias: myeloproliferative neoplasms, 2023:
- To diagnose suspected myeloproliferative neoplasms, bone marrow (BM) smears and trephine biopsies should be collected at time of diagnosis, or within a short timeframe thereafter, and in the absence of active therapy, especially with cytoreductive drugs.