Localization Before Diagnosis: A Physiology-First Approach to Thrombocytopenia
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
When clinicians encounter thrombocytopenia, the reflex is often to ask: What causes this?
The instinct is understandable. Medicine trains us to think in diagnoses. Physiology asks a different first question:
Where is the platelet deficit generated?
Thrombocytopenia is not fundamentally a diagnosis. It is a disturbance in platelet homeostasis. Physiologic disturbances are best understood not by naming them, but by localizing them. Diagnosis is not the beginning of reasoning. It is the endpoint of successful localization.
Two ways clinicians actually reason
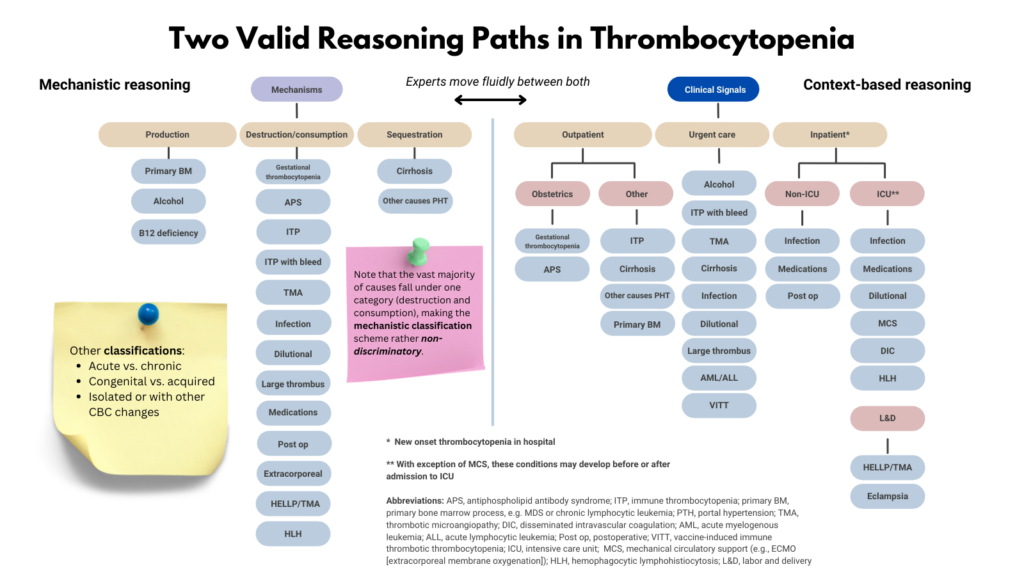
In practice, clinicians use two complementary modes of reasoning when approaching thrombocytopenia. One is contextual pattern recognition. The other is mechanistic localization. These are not competing strategies. They are layers of the same process.
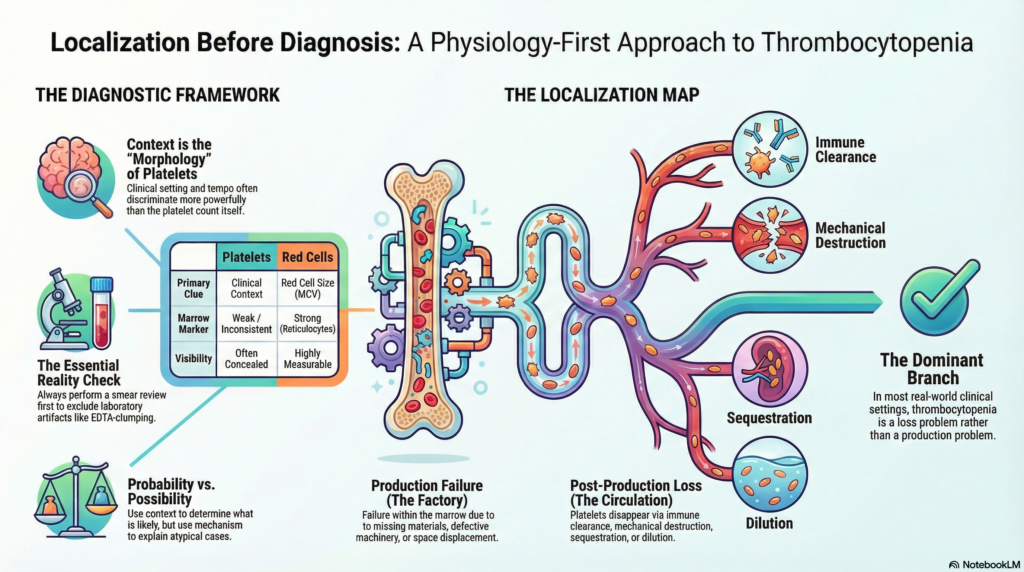
Context is the visible layer. Thrombocytopenia rarely presents with intrinsic morphologic patterns the way anemia does. Instead, it presents with contextual patterns: where the patient is, how sick they are, what medications they are receiving, and how quickly the platelet count is falling. These often discriminate more powerfully than the count itself.
In platelet disorders, context functions as morphology.
Mechanistic reasoning operates at a deeper level. Instead of asking what diagnosis fits the number, the clinician asks where platelets are failing within their lifecycle. Are they not being produced? Are they leaving circulation prematurely?
Experienced clinicians often perform this step implicitly. Teaching requires making that hidden reasoning visible.
An important asymmetry
There is an important asymmetry between thrombocytopenia and anemia. In anemia, the first pattern signal is red cell size, reflected in the MCV. In thrombocytopenia, the first pattern signal is clinical setting.
In anemia, a single test, the reticulocyte count, provides a powerful early physiologic branch point separating production failure from peripheral loss. In thrombocytopenia, no equivalent test cleanly distinguishes these domains in real time. Production and removal often blur together. Laboratory markers rarely separate them decisively.
Red cell physiology exposes itself to measurement. Platelet physiology often does not. The diagnostic tools differ. The physiologic logic does not.
Why context works so well
Context-based reasoning succeeds most of the time because platelet disorders cluster strongly by clinical environment. Hospitalized patients often develop thrombocytopenia from systemic illness, medications, or consumptive processes. Outpatients with isolated thrombocytopenia frequently have immune-mediated disease or drug effects. Pregnancy, infection, critical illness, and chronic liver disease each shift probability toward particular mechanisms.
Platelet disorders are therefore more context-dependent than red cell disorders. Location of care, tempo of decline, medications, comorbid illness, and systemic findings often discriminate more effectively than mechanism alone. Context frequently supplies the first narrowing step. Physiology then refines it.
This is especially true in isolated thrombocytopenia, where most real-world cases arise from post-production mechanisms such as immune removal or consumption. When the majority of patients occupy the same physiologic branch, that branch loses early discriminatory value. Context then becomes the more informative signal.
Acknowledging this is not a concession. It is an honest description of clinical reality.
Platelet counts rarely localize physiology. Clinical setting often does.
What makes thrombocytopenia different from anemia
The difference is not biologic complexity. It is physiologic visibility. Some systems expose their failures clearly. Others conceal them.
| Feature | Platelets | Red cells |
|---|---|---|
| Reliable marrow response marker | weak | strong |
| Destruction markers | nonspecific | specific |
| Production rate measurable | limited | robust |
| Mass measurement | difficult | feasible |
Mechanistic reasoning works best when physiology is measurable. Anemia is unusually well suited to a physiology-first approach. Thrombocytopenia obeys the same biologic principles, but its signals are less legible.
The limitation is not conceptual. It is observational.
Each cytopenia therefore announces itself through a different first clue:
| Cytopenia | First pattern signal |
|---|---|
| Anemia | red cell size |
| Thrombocytopenia | clinical context |
| Neutropenia | tempo and infection pattern |
The physiology is unified. The entry signal differs.
The physiologic map
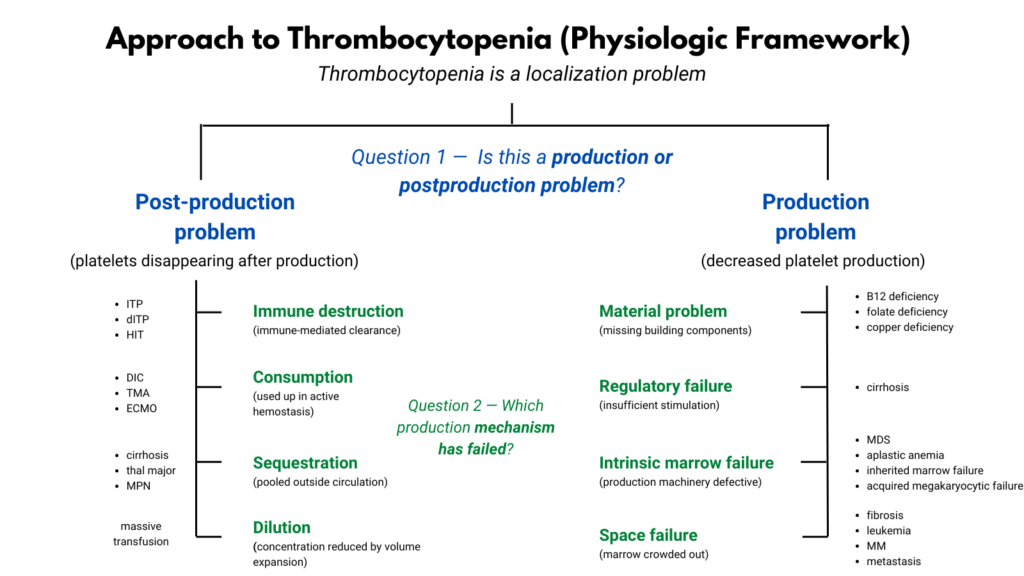
The first task is not to name a disease. It is to determine which stage of the platelet lifecycle is failing.
Thrombocytopenia occupies two primary physiologic domains:
Production failure — platelets are not generated adequately in the marrow.
Post-production loss — platelets leave circulation prematurely or their effective concentration falls.
These are not diagnoses. They are failure modes.
The purpose of this map is not to rank likelihood. It is to define what is biologically possible. Probability reshapes the map. It does not replace it.
The first branch point is not mechanism. It is reality.
Before localization can begin, thrombocytopenia must be confirmed as real.
Platelets are uniquely vulnerable to laboratory artifact. EDTA-related clumping, satellitism, and handling effects can produce falsely low counts. A smear review is therefore not ornamental. It is the earliest physiologic checkpoint available.
This step sits outside physiology. Pseudothrombocytopenia is not a disease state but a measurement artifact. Like spurious hyperkalemia or pseudohyponatremia, it must be excluded before physiologic reasoning begins.
Where platelets go after they are made
If thrombocytopenia is real, localization proceeds within the physiologic map.
Post-production loss may occur through:
- immune clearance
- mechanical destruction
- consumptive coagulopathy
- splenic sequestration
- dilution
These differ biologically but share one defining physiologic property: platelets disappear after entering circulation.
Production failure reflects dysfunction within the marrow system itself. Production may falter because:
- required materials are missing
- regulatory stimulation is inadequate
- megakaryocytic machinery is defective
- marrow space is displaced
Again, these are organizing domains, not diagnoses.
What different tests actually do
Not all tests answer the same question. Diagnostic studies contribute at different levels of reasoning:
- Some confirm reality.
- Some localize failure broadly.
- Others localize it more precisely.
- A few name the disease.
Seen this way, early testing functions as physiologic interrogation.
| Test | Role | What it reveals |
|---|---|---|
| Peripheral smear | reality check + localization clues | clumping, fragmentation, dysplasia |
| Coagulation studies | consumption probe | systemic platelet use |
| Other cell lines | production probe | isolated vs marrow-wide failure |
| Medication timeline | probability modifier | drug-mediated processes |
| Bone marrow exam | mechanism confirmer | factory integrity |
Tests do not simply diagnose disease. They progressively constrain physiology.
Possibility versus probability
Mechanistic frameworks describe what is biologically possible. Clinical reasoning must also account for what is statistically likely.
A physiologic diagram is a possibility map. It shows every mechanism capable of lowering platelets. But when a clinician evaluates a real patient, probability reshapes that landscape immediately.
Mechanisms remain constant. Probabilities shift with context.
Diagnostic error arises when possibility maps are mistaken for probability maps.
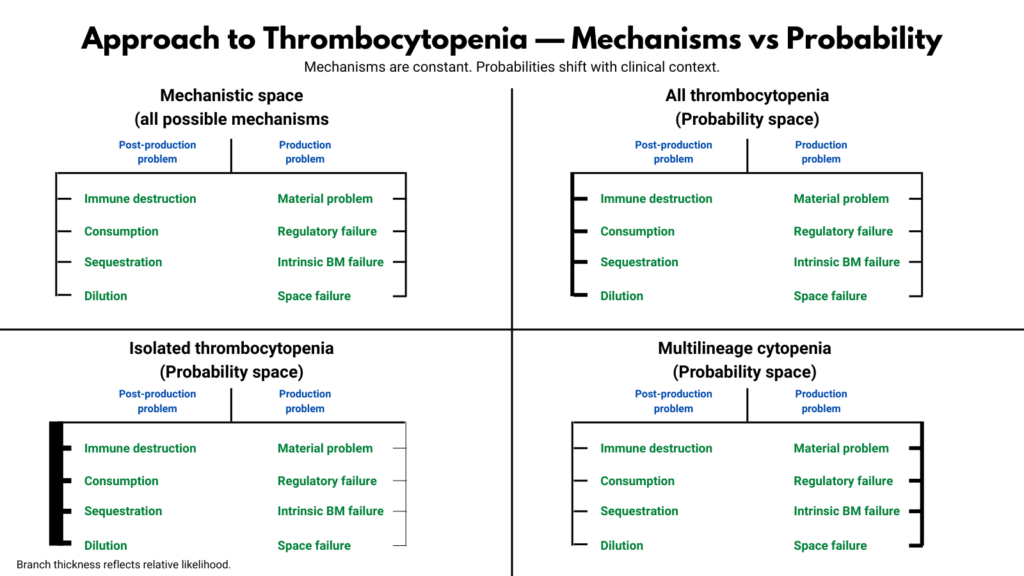
Why post-production mechanisms dominate clinically
Platelet turnover is rapid. Peripheral removal can therefore produce dramatic count reductions within hours or days. Immune clearance, consumption, or sequestration may generate abrupt thrombocytopenia despite otherwise preserved hematologic indices.
Production failure often declares itself differently. Additional cytopenias, smear abnormalities, systemic illness, or gradual decline frequently accompany impaired platelet generation.
In most real-world settings, thrombocytopenia is more often a loss problem than a production problem.
This is a probability statement, not a mechanistic one.
Why mechanism still matters
If probability often points in the right direction, why think mechanistically at all?
Because probability is directional, not structural. It suggests where to look. It does not explain what is happening.
Mechanistic reasoning accomplishes things pattern recognition cannot:
- it explains why findings occur
- it unifies diverse diseases under shared principles
- it clarifies atypical presentations
- it prevents premature closure
- it stabilizes reasoning when data conflict
Pattern recognition manages routine cases. Mechanism rescues difficult ones.
Expertise does not require thinking mechanistically all the time. It requires knowing when to shift.
A case where mechanism overrides context
An outpatient presents with isolated severe thrombocytopenia. Context suggests immune thrombocytopenia. Steroids are given. The platelet count does not respond. Second-line therapy is tried. The count remains below 10.
At this point, probability has stopped explaining the data.
Bone marrow examination shows absent megakaryocytes. The problem is not peripheral destruction. It is production failure.
Context pointed in one direction. Physiology redirected the map.
A practical synthesis
In real clinical practice, thrombocytopenia is often approached through context first. This is appropriate. Context rapidly reshapes probability and often identifies the correct pathway before formal localization is articulated.
Real diagnostic reasoning usually unfolds through some combination of:
context → pattern → mechanism → diagnosis
Each step refines the last. None replaces the others.
Mechanistic frameworks are not primarily bedside algorithms. They are cognitive scaffolds. Most thrombocytopenia can be managed correctly using context and pattern recognition alone. But when findings conflict, when presentations are atypical, or when stakes are high, mechanism becomes indispensable.
A final principle
Thrombocytopenia is best approached by asking where platelet homeostasis is failing rather than by reciting a flat list of causes, with clinical context playing the role that morphology plays in anemia.
Good clinicians do not begin by naming diseases. They begin by locating failures. Ordering tests is therefore not mere data gathering. It is physiologic interrogation.
Context suggests direction.
Mechanism supplies structure.
Diagnosis concludes.
Synthesis: how to actually practice with this model
Let context start the evaluation because it is fast and reflects how platelet disorders present clinically.
Confirm thrombocytopenia is real before localizing physiology, since platelets are uniquely vulnerable to laboratory artifact.
Localize the deficit to lifecycle stage: production failure or post-production loss.
Within the chosen branch, use targeted data to refine localization.
Other cytopenias suggest marrow production problems.
Coagulation abnormalities suggest consumptive loss.
Smear findings may reveal mechanism.
Switch from context to physiology the moment the clinical picture and the data diverge.
Remember that good clinicians begin by locating failures, not naming diseases; diagnosis is the endpoint of structured localization, not its substitute.