Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
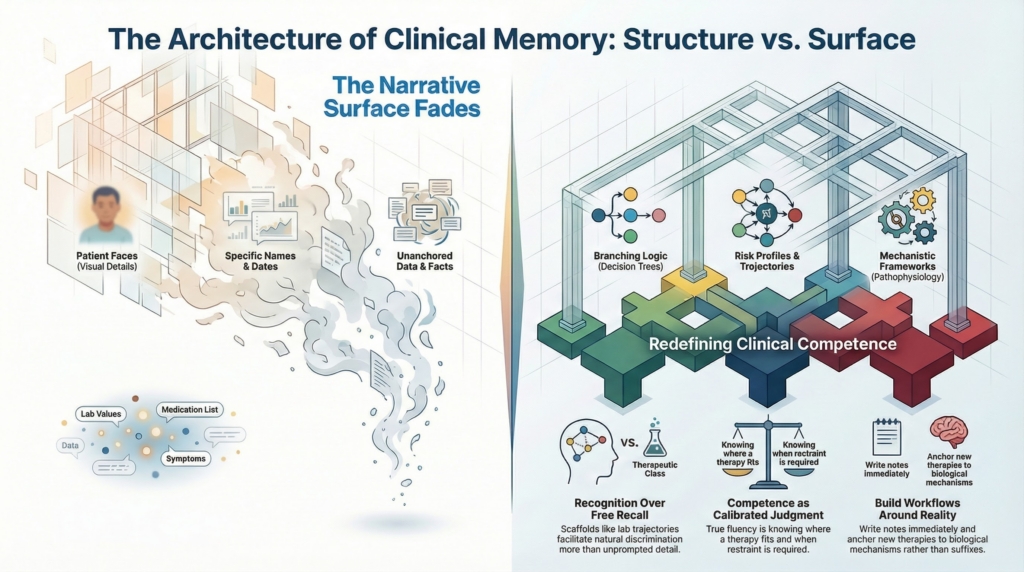
As narrative elements fade, enduring diagnostic frameworks, mechanistic logic, and risk trajectories remain accessible. Clinical competence therefore depends less on recall than on the architecture that organizes understanding.
What Fades
A patient once returned to clinic, sat down, and began speaking as if we were resuming a conversation.
I nodded. I listened. I tried to orient myself.
Within a few minutes it became clear we were not meeting for the first time: I had examined him, written a note, made recommendations — and I remembered none of it.
When I opened the chart, the structure came back immediately: the hemoglobin trend, the ferritin, the rationale for intravenous rather than oral iron.
His face did not.
This is not new. It has always been true.
If I do not write my note soon after seeing a patient, the encounter begins to dissolve. Within hours the visual details begin to blur. But I will remember the diagnostic frame. I will remember the branching logic of the differential. I will remember why one option carried more risk than another.
I remember frameworks far more vividly than I remember faces.
I see the same pattern when I read fiction. I can be halfway through a novel and come across a name I should recognize, only to realize I no longer remember who that person is. I turn back and reread. The prose is familiar, but the map of who belongs where is not. I can watch a film and, a week later, struggle to recount the plot or retrieve the title.
Detail slips quietly away.
The narrative surface fades.
The structure remains.
Recognition and Recall
For years I interpreted this pattern as deficiency.
In conference, fellows introduce newer agents — often monoclonals whose names all seem to end the same — and their suffixes blur together in my mind. The mechanism may not immediately surface. The name may hover just out of reach. In those moments comes a brief flicker of exposure — I should know this — followed by a quiet internal decision: acknowledge it inwardly or let it pass.
The same pattern appears elsewhere. In medical school I performed better on multiple-choice examinations than on essay exams. Recognition has always come more easily to me than free recall. Present me with a scaffold — a chart, a lab trajectory, a therapeutic class — and discrimination feels natural. Ask me for unprompted detail and I hesitate.
Until I can place a new therapy on a mechanistic map, its name tends to hover at the edge of recall.
Many clinicians retrieve detail with impressive fluency. Some hold detail and structure with equal ease. Others lean more heavily toward one or the other. These differences are variations in emphasis, not measures of worth — though medicine often forgets that.
Architecture
Over time I have come to understand that my mind privileges structure.
If a fact bolts onto a conceptual scaffold, it stays. If it hangs in midair, it drifts.
Say “JAK inhibitor” or “anti-CD20” and the downstream pathways and risk profiles eventually come into focus, even if the brand name stalls. The class connects to mechanism, the mechanism to risk, the risk to decision. The architecture is intact even when the label hesitates.
There is vulnerability in acknowledging that not every entry point is immediately accessible. Authority in medicine often signals itself through rapid recall. Speed looks like fluency, and fluency like wisdom, even when it is mostly rehearsal.
But competence in clinical practice is not encyclopedic storage.
It is calibrated judgment.
It is knowing where a therapy fits, when it shifts risk, and when restraint is wiser than action. It is the ability to think clearly even when words arrive a beat late.
Building Around It
Eventually I stopped trying to reshape my mind into a perfect recall machine it is not.
I write notes soon after visits because I understand how encoding works for me. I anchor new therapies to mechanisms rather than suffixes. When necessary, I say, “Remind me which pathway that targets,” and then think from there. I build my workflow around that reality, not against it.
What I cannot reliably retrieve are faces, plot lines, or movie titles.
I am still learning to live with that.
What I try not to forget is how to think.
That’s what I hang on to.