When the question becomes the test
Two examiners stand at the bedside.
White coats, unreadable expressions.
“Dr. Aird, please examine this patient for an MCV of 140.”
A pause.
The setting
In Canadian medical training, the oral examination is a rite of passage.
There are two formats: the long case and the short case. The long case allows time to gather a history, examine the patient, and present a structured assessment. The short case is something else entirely.
It is compressed. Exposed. Unforgiving.
You are brought to the bedside and given a task, often framed in an unusual way, and expected to proceed immediately, under observation, while thinking out loud. Not just to perform, but to reveal how you organized your thinking in real time.
This was my short case.
The question
What does it mean to “examine a patient for an MCV of 140”?
The instruction is deliberately incomplete. It does not tell you where to begin or what to look for. It offers no script.
In that moment, you are not being tested on what you know.
You are being tested on how you organize what you know.
From differential to examination
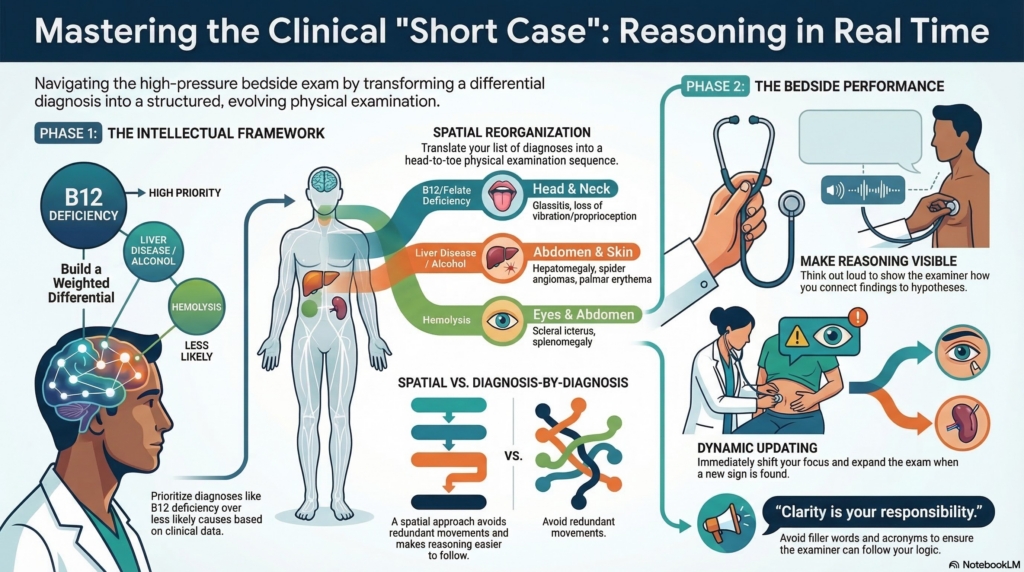
The first step is straightforward. An MCV of 140 invites a differential: vitamin B12 or folate deficiency, reticulocytosis from hemolysis, liver disease and alcohol use, hypothyroidism, medication effects such as hydroxyurea, and less commonly a primary bone marrow disorder.
But not all differentials carry equal weight.
An MCV of 140 is not simply macrocytosis. It is extreme. Many common causes of mild macrocytosis, such as reticulocytosis or hypothyroidism, rarely reach this level. Reticulocytosis contributes to macrocytosis, but rarely drives an MCV to 140 on its own.
Before the examination begins, the probabilities are already shifting.
Medication effects, particularly hydroxyurea, and severe megaloblastic processes such as pernicious anemia move to the foreground. Other possibilities recede.
Rarely, an extreme MCV may reflect a laboratory artifact, as in cold agglutinin disease, where red cell clumping falsely elevates the measured value. This cannot be confirmed at the bedside, but remains a consideration when confronted with a value in this range.
The differential is not just a list.
It is a weighted list.
The challenge comes next.
Once the differential is formed, the problem is not what to think, but how to proceed.
There are at least two ways to proceed.
One is to take each diagnosis in turn and examine for its associated findings. This approach is logically sound. It reflects a direct mapping from disease to finding. But at the bedside it fragments the examination. You move back and forth across the body, following diagnoses rather than structure. The logic is intact, but the execution is difficult to follow.
The other approach is to reorganize the differential spatially.
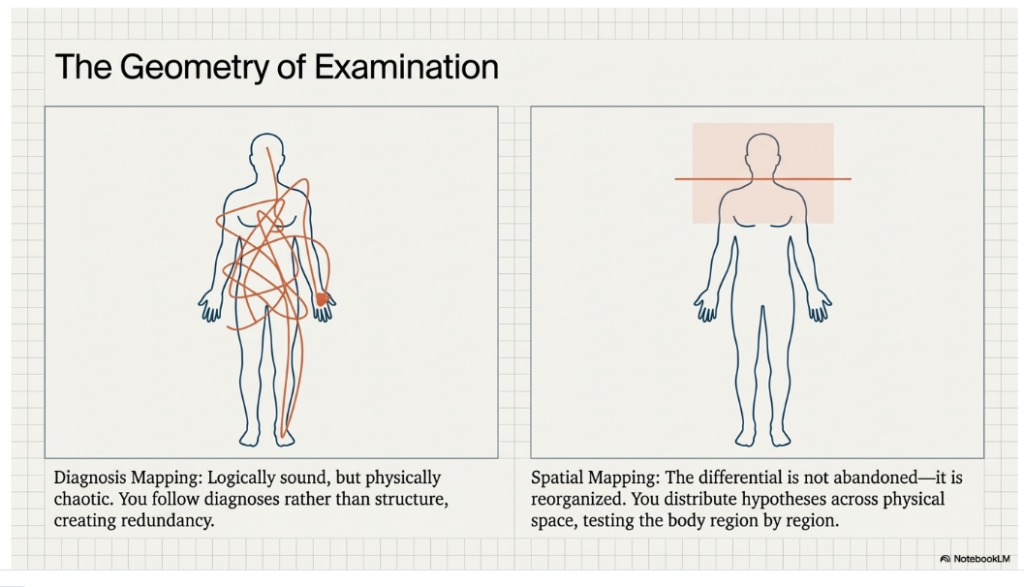
You begin with the head and neck, asking what each diagnosis would look like there. Conjunctival pallor for anemia. Scleral icterus for hemolysis or liver disease. Glossitis for a megaloblastic process. You then move down the body, region by region, redistributing the differential across physical space. The hands become a place to look for palmar erythema or Dupuytren’s contractures. The chest for spider angiomas and gynecomastia. The abdomen for hepatomegaly or splenomegaly. The nervous system for loss of vibration or proprioception.
The differential is not abandoned.
It is reorganized.
Each region of the body becomes a testing ground for multiple hypotheses, not just a checklist of signs. A single finding can inform several diagnoses at once, allowing hypotheses to be tested in parallel rather than in sequence. By contrast, a diagnosis-by-diagnosis approach introduces redundancy, requiring repeated passes through the same regions of the body.
In principle, both approaches are valid.
In practice, the spatial approach is more effective at the bedside. It imposes order on the examination, makes your reasoning easier to follow, and allows multiple hypotheses to be tested efficiently within a single pass through the body.
At first glance, this can look like recall. The differential is familiar. The mapping can be rehearsed. With enough repetition, the sequence itself can become automatic.
But the examination does not unfold in a vacuum.
It responds.
You look at the eyes and see scleral icterus. Although hemolysis and liver disease were less likely given the degree of macrocytosis, they were never excluded. A specific finding can rapidly restore a receded diagnosis.
You pause longer at the abdomen, specifically assessing for hepatomegaly and splenomegaly.
You test vibration in the toes and find it reduced. Now B12 deficiency moves forward, as posterior column involvement is more characteristic of vitamin B12 deficiency than folate deficiency. The neurologic examination expands. Reflexes matter more.
Each finding reshapes the differential. Each step in the examination is influenced by the last.
The sequence is structured, but the reasoning is dynamic.
Naming possibilities is memory.
Updating them in real time is reasoning.
At the bedside
The task is not simply to move from head to toe. It is to make your reasoning visible as you go.
“I have been asked to examine this patient in the context of a markedly elevated MCV.
My differential diagnosis includes megaloblastic processes such as vitamin B12 or folate deficiency, medication effects such as hydroxyurea, liver disease and alcohol use, hypothyroidism, and reticulocytosis from hemolysis.
Given the degree of macrocytosis, I am particularly attentive to medication effects and megaloblastic processes, while also assessing for other potential causes.
I will perform a focused examination, moving from head to toe, looking for findings that help distinguish among these possibilities.
I am starting with the head and neck, looking for conjunctival pallor, scleral icterus, and glossitis.”
A pause.
“There is scleral icterus.”
The differential shifts.
“I will focus on the abdomen, assessing for hepatomegaly and splenomegaly, given the possibility of hemolysis or liver disease.”
Later:
“Vibration sense is reduced.”
Another shift.
“I will expand the neurologic examination, given concern for vitamin B12 deficiency.”
At the end of the examination:
“Taken together, these findings would prioritize vitamin B12 deficiency, while keeping liver disease or hemolysis in consideration depending on the full clinical context.”
The examination is not a script.
It is a series of adjustments.
The performance
The short case is not only a test of reasoning.
It is a test of expression.
You are expected to think out loud, but not to think chaotically.
Hesitation is inevitable, but filler is not your friend. Every “um” fragments the signal. Acronyms, unless universally understood, obscure rather than clarify. The examiner is not inside your head. Clarity is your responsibility.
You begin by framing the problem.
You declare your approach.
You move through the body with purpose.
You connect findings to hypotheses.
The goal is not to sound impressive.
It is to be understandable.
The short case tests not only how you think, but how cleanly your thinking can be heard.
What is the point?
It is fair to ask what any of this achieves.
The short case is artificial. The setting is stressful. It may select for composure as much as reasoning. It may disadvantage quieter trainees. It may reward fluency over depth.
These are real limitations.
But the format does something that is otherwise difficult to see.
It makes reasoning visible.
Not the polished version presented after the fact, but the unfolding process itself. The moment when one finding reshapes the differential. The decision to linger, to redirect, to test a different hypothesis.
In most clinical settings, this process is hidden. We think privately and present conclusions.
The value of the short case is not that it is fair.
It is that it reveals.
The process is the performance.
Closing
You are examining your hypotheses through the patient.
The short case may be imperfect.
But it captures something real:
the moment when thinking must become action.
From diagnosis to physical findings
This reasoning can be made explicit.
Vitamin B12 deficiency (pernicious anemia)
- pallor
- scleral icterus (ineffective erythropoiesis)
- glossitis
- impaired vibration/proprioception
- ataxia
Liver disease / alcohol-related
- jaundice
- spider angiomata
- palmar erythema
- hepatomegaly
- gynecomastia
- Dupuytren’s contracture
Hypothyroidism
- dry skin
- bradycardia
- delayed reflex relaxation
- periorbital puffiness
Reticulocytosis / hemolysis
- jaundice
- splenomegaly
Medications (e.g., hydroxyurea)
- leg ulcers
- hyperpigmentation (skin/nails)
- often no specific physical findings
Primary bone marrow disorders (e.g., MDS)
- pallor or bruising depending on cytopenias
- often no specific physical findings
From findings to the body
This information can then be reorganized spatially.
General
- pallor
- jaundice
Eyes
- scleral icterus
- periorbital puffiness
Mouth
- glossitis
Skin
- spider angiomata
- palmar erythema
- dry skin
- leg ulcers
- hyperpigmentation (skin/nails)
Chest
- gynecomastia
Cardiovascular
- bradycardia
Abdomen
- hepatomegaly
- splenomegaly
Neurologic
- impaired vibration/proprioception
- ataxia
- abnormal reflexes