Why questioning in medical training becomes either a scaffold for thought or a stage for hierarchy
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
In some training environments, rapid-fire questioning is ordinary.
In others, it is suspect.
Sometimes it is defended as rigor.
Sometimes condemned as humiliation.
Often it is reduced to caricature.
What gets lost is something more interesting.
The question is one of the oldest tools in medical education.
How it is held determines whether it sharpens thinking or displays power.
One tool, different contracts
In Canadian training culture, at least in the programs I observed, oral examination is explicit.
Trainees know they will be questioned.
They know they will be interrupted.
They know they will be pushed to think aloud.
Questioning is normalized as evaluation.
It is expected.
It is practiced.
It is culturally legible.
In much of American training culture, the same behavior is read differently.
Questioning is often interpreted as:
being put on the spot
being challenged publicly
being exposed
The same act can feel pedagogical in one system
and adversarial in another.
This is not about personality.
It is about training architecture.
When the tool becomes the threat
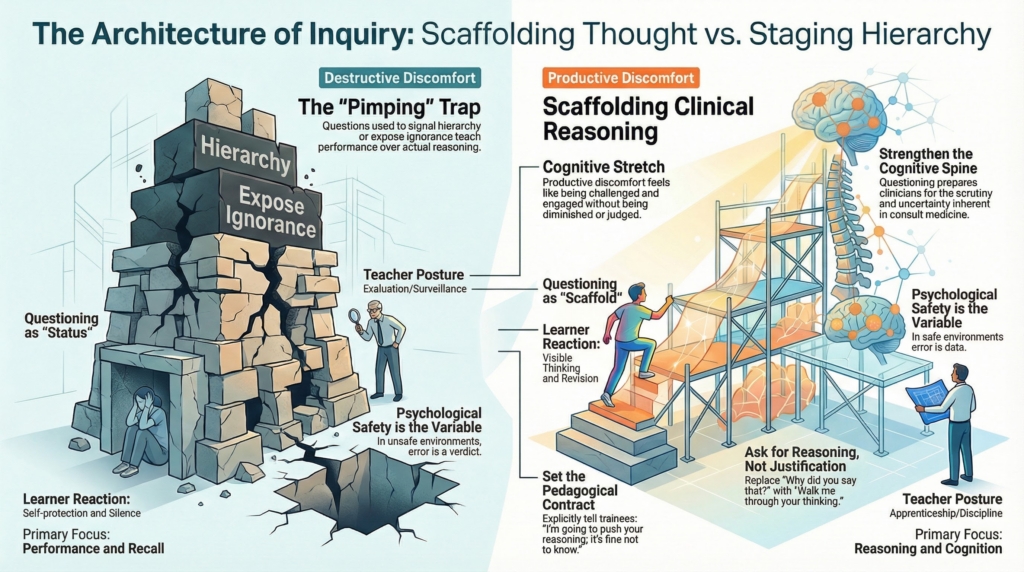
“Pimping” became a loaded word not because questioning is inherently harmful, but because it has often been used for other purposes:
to display superiority
to signal hierarchy
to expose ignorance for social effect
In those settings, the function of the question shifts. It no longer probes reasoning. It performs status.
Trainees learn the hidden curriculum:
answer correctly or lose standing
hesitate and be judged
think aloud and risk embarrassment
This teaches performance, not reasoning.
Why questioning works
Used well, questioning is one of the most powerful cognitive tools in medicine.
It forces articulation of thinking.
It reveals assumptions.
It allows correction in real time.
It makes reasoning visible.
Consult work is not recall.
It is judgment under uncertainty.
It requires:
framing
weighting
recognizing uncertainty
naming tradeoffs
These are learned through dialogue.
Not monologue.
Why the problem persists
The misuse of questioning did not arise from a few harsh personalities. It emerged from structure.
Ward rounds are public, time-pressured, hierarchical, and evaluative. Attendings are rarely trained to teach. Assessment is constant. Authority is asymmetrical.
Under those conditions, questioning drifts toward performance testing because performance is what the environment rewards.
The problem is not that teachers are harsh.
It is that the system quietly incentivizes harshness.
The missing architecture: safety
The decisive variable is psychological safety.
In environments with it, trainees learn:
being wrong is part of learning
thinking aloud is expected
uncertainty is permissible
Without it, they learn:
wrong answers are dangerous
silence is safer than speculation
visibility invites risk
The same technique produces opposite outcomes because the meaning of error changes.
In one system, error is data.
In another, it is verdict.
Why it often feels threatening
In many U.S. programs, public questioning is tightly tied to evaluation.
It carries associations with:
documentation
grading
formal consequences
power asymmetry
The trainee does not hear:
Let’s think together.
They hear:
You are being judged.
Even when intent is good.
What productive discomfort actually feels like
There is a kind of discomfort that builds clinicians.
It is not humiliation.
It is cognitive stretch.
It feels like being asked a question you cannot answer immediately, beginning to reason aloud, realizing your first frame is incomplete, revising it, and sensing your understanding reorganize in real time.
You feel exposed, but engaged.
Pressed, but not diminished.
Challenged, but not judged.
That is how clinical reasoning matures.
Destructive discomfort feels different. Attention shifts from the problem to the evaluator. Thinking narrows. Risk-taking stops. The goal becomes self-protection.
Both involve pressure. Only one produces growth.
Why abandoning questioning is a loss
In response to harmful questioning cultures, some educators minimize questions altogether. They lecture instead.
Something important is lost.
Without questioning:
thinking stays hidden
assumptions go untested
errors surface later
judgment remains untrained
Trainees may feel safer. They are often less prepared.
Consult medicine is scrutiny.
The real skill
The solution is not to eliminate questioning. It is to hold it differently.
Effective teachers signal the frame before the first question:
I’m going to push your reasoning.
It’s fine not to know.
Talk me through your thinking.
They model uncertainty. They correct without spectacle. They pursue reasoning rather than answers.
The question becomes a scaffold, not a trap.
The uncomfortable truth
Consult medicine requires intellectual toughness.
Not bravado. Not humiliation.
But the ability to reason under questioning.
Comfort with uncertainty.
Capacity to think aloud.
Willingness to be wrong and revise.
A culture that removes all strain does not prepare trainees for real consult life.
The task is not to eliminate pressure.
The task is to make pressure educational.
What this teaches about consult culture
The debate over pimping is not really about manners.
It is about how medicine teaches thinking.
Whether it trains performance or reasoning.
Whether it rewards polish or revision.
Whether it treats uncertainty as failure or as signal.
Consult Practice belongs firmly in the camp of visible thinking.
Visible thinking requires questions.
Questions create pressure.
Pressure requires trust.
The goal is not to toughen trainees emotionally.
The goal is to strengthen their cognitive spine.
That happens through questioning.
As training.
As discipline.
As respect for the work’s seriousness.