When rules bend and judgment matters most
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
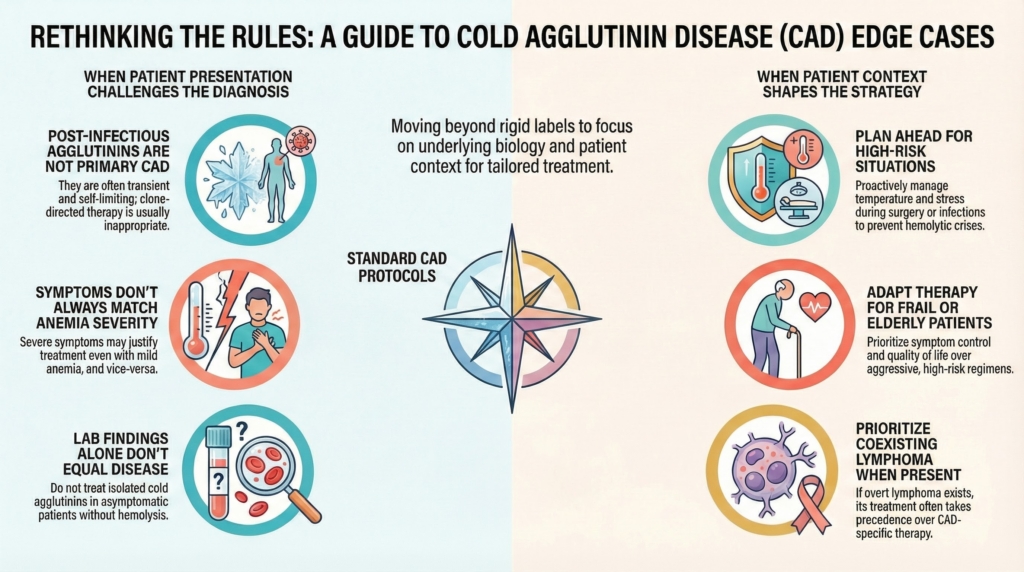
Cold agglutinin disease follows recognizable biological patterns, yet real-world practice is often defined by exceptions, overlaps, and context-dependent behavior. Major reviews emphasize that atypical presentations, mixed immune mechanisms, and secondary forms are common and require clinicians to interpret disease through mechanism and trajectory rather than diagnostic labels alone.1
Contemporary frameworks also emphasize that CAD is not only an autoimmune hemolytic anemia, but a marrow-based clonal B-cell disorder and monoclonal gammopathy of clinical significance, reinforcing why mechanism—not label—must guide decisions.2
Management in CAD is therefore guided by dominant mechanism, disease trajectory, and patient impact—not by diagnostic labels alone.
Edge cases are not failures of classification. They are where classification must be interpreted—testing whether decisions are driven by biology, tempo, and patient impact rather than reflex adherence to category.
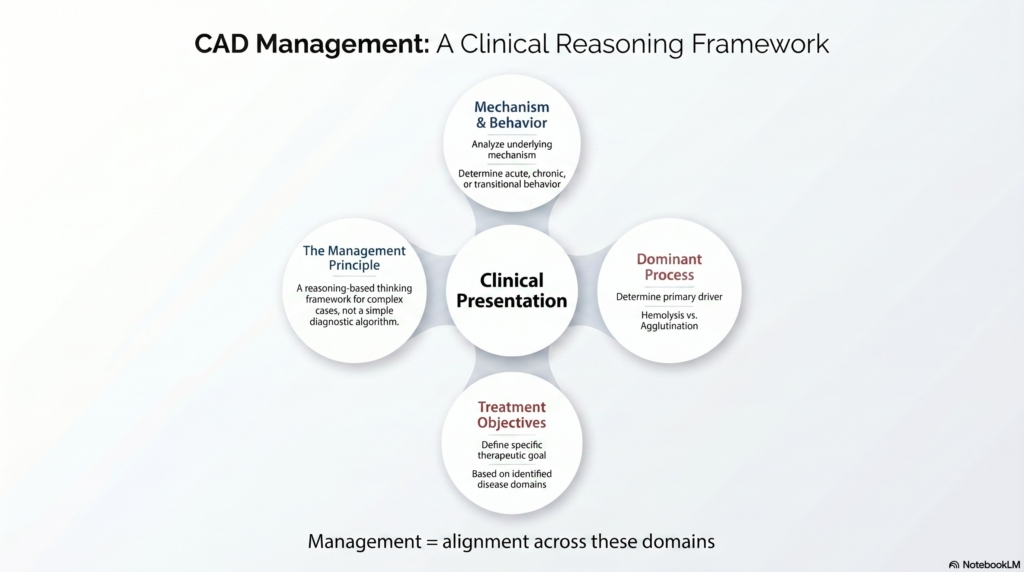
A reasoning framework for unexpected presentations
When a presentation does not fit neatly, four questions stabilize clinical thinking:
- Is this truly CAD or a mimic?
- What mechanism is dominant right now?
- Is the disease behavior acute, chronic, or transitional?
- Does the treatment goal match the patient’s current reality?
The sections that follow are not a catalog of exceptions. They are demonstrations of these questions in action.
Post-infectious cold agglutinins
Cold agglutinins frequently arise after infection and are not equivalent to primary CAD. They are usually transient, polyclonal, and self-limited, often associated with organisms such as Mycoplasma pneumoniae or Epstein–Barr virus, and typically lack an underlying clonal B-cell disorder.3
Clinical implications:
- observation is usually appropriate
- clone-directed therapy is generally not indicated
- disease-directed treatment is often not required
Misclassification of transient post-infectious hemolysis as chronic CAD risks unnecessary long-term therapy.4
Framework application
Here, the mechanism is transient, the disease behavior is acute and self-limited, and the treatment goal is stabilization rather than suppression.
Each scenario that follows can be read through this same lens: mechanism, tempo, and treatment goal.
Isolated cold agglutinins without hemolysis
Cold agglutinins may be detected incidentally during preoperative testing or blood bank evaluation.6
Core principle
Do not treat laboratory findings in isolation.
Disproportionate symptoms with modest anemia
Symptom burden correlates imperfectly with hemoglobin level.7
Circulatory manifestations such as acrocyanosis, cold-induced pain, and color change arise primarily from cold-induced IgM-mediated red-cell agglutination in acral circulation rather than from anemia itself, and in some patients may be amplified by coexistent cryoglobulin activity.8
Treatment may be appropriate despite relatively preserved hemoglobin when circulatory symptoms are disabling or anemia is symptom-producing.
Management requires:
- explicit symptom assessment
- avoidance of rigid numeric thresholds
- alignment of therapy with functional impact
Severe anemia with limited symptoms
Clinical impact does not always track a single hemoglobin value, and treatment decisions should incorporate trajectory, hemolysis burden, symptoms, and comorbidity.9
Implications:
- urgency should reflect trajectory, not a single value
- treatment must be individualized
- absence of symptoms does not mandate therapy
The number alone does not define severity.
Acute hemolytic exacerbations
Hemolytic exacerbations may be precipitated by infection, cold exposure, or major physiologic stressors, reflecting amplification of classical complement activation.10
Important distinction:
Acute worsening does not automatically indicate treatment failure.
Supportive care and reassessment after stabilization may be sufficient.
This reflects disease biology, not necessarily therapeutic failure.
Urgent transfusion scenarios
Urgent transfusion should not be withheld when clinically necessary. In CAD, close communication with transfusion services, warming measures, and careful temperature management are essential; compatibility testing may require modified handling, but life-saving transfusion should proceed with appropriate precautions rather than be delayed.
Perioperative and procedural settings
Procedures introduce unique risk because hypothermia promotes cold-antibody binding, red-cell agglutination, and downstream complement activation, which can exacerbate hemolysis.11
Practical requirements:
- strict temperature control
- coordination with anesthesia teams
- advance transfusion planning
Thermal protection is a core disease-management measure intended to reduce cold-triggered agglutination and downstream hemolysis. Failure to anticipate this risk has been associated with severe exacerbations.12
Pregnancy and reproductive considerations
CAD in pregnancy is rare and evidence is limited.13
Management typically emphasizes:
- supportive care
- transfusion if necessary
- close monitoring
Rituximab-based regimens and cytotoxic therapies are generally avoided during pregnancy, and experience with complement inhibitors remains limited. Decisions therefore prioritize maternal stability, fetal safety, and thermal protection unless anemia becomes severe or rapidly progressive.
Current evidence does not support standardized treatment algorithms, so decisions must be individualized.
Frail or elderly patients
Many patients with CAD are older and have comorbidities.14
Priorities often shift:
- minimizing immunosuppressive toxicity
- preserving function
- prioritizing quality of life
The biologically strongest therapy may not be clinically appropriate if the patient cannot safely absorb its risks.
Coexisting lymphoproliferative disease
Primary CAD commonly arises from an indolent clonal B-cell disorder.15
When overt lymphoma is present, lymphoma-driven indications may supersede hemolysis-driven ones, and therapy may be selected primarily for malignancy control.16
Discordance between lymphoma response and hemolysis response should prompt reassessment of mechanism rather than automatic escalation.
Mixed or atypical autoimmune hemolysis
Some patients exhibit mixed immune mechanisms, including IgG- and complement-mediated hemolysis or atypical DAT patterns.17
These cases require:
- reassessment of mechanism
- iterative therapy adjustments
- acceptance that full normalization may be unrealistic
Determining whether an IgG-mediated component is present may materially affect treatment selection; by contrast, corticosteroids should generally not be used for typical CAD.
Partial control may represent success.
Pre-analytical laboratory artifacts from cold samples
Cold-dependent agglutination can produce spurious laboratory results such as elevated MCV, low RBC count, and high MCHC that correct when samples are warmed.18
This pattern itself can be a diagnostic clue.
Laboratory data that do not match the clinical picture should always be verified with warmed samples before clinical decisions are made.
Refractory or partial responders
Failure to normalize values does not necessarily indicate treatment failure.
Recommended reassessment:
- confirm diagnosis and dominant mechanism
- exclude secondary triggers
- reassess treatment goals
Partial disease control may represent success when biology or patient factors limit achievable outcomes.19Berentsen S. Novel insights into the treatment of cold agglutinin-mediated autoimmune hemolytic anemia. Therapeutic Advances in Hematology. 2019.[/efn_note
Explicit principle
Edge cases are not failures of the framework.
They are where the framework proves its value.
Expert CAD management recognizes:
when rules apply
when they bend
when they must be set aside
and replaces rigid algorithms with mechanism-based reasoning, longitudinal judgment, and patient-centered goals.
Reflect and Apply
When a CAD presentation does not fit the usual pattern, pause before reaching for the next treatment.
Ask:
What mechanism is dominant right now?
Complement-mediated hemolysis, cold-induced agglutination, secondary infection, overt lymphoma, mixed AIHA, or laboratory artifact?
What is the tempo?
Transient, chronic, accelerating, perioperative, pregnancy-associated, or treatment-refractory?
What is the goal of treatment?
Stabilization, symptom control, prevention of cold-triggered worsening, lymphoma control, or long-term disease modification?
In edge cases, the safest question is often not “What category does this patient fit?” but:
What problem am I actually trying to solve?
Test your thinking
A short, judgment-focused quiz on special situations and edge cases in cold agglutinin disease.