It has long been held that hypothyroidism (and possibly hyperthyroidism) may lead to anemia. Thyroid function measurements are often included in the work up of anemia. However, a critical appraisal of the literature reveals that thyroid dysfunction is a RARE cause of anemia.
A) Let’s look at the data from the anemia –> thyroid dysfunction angle
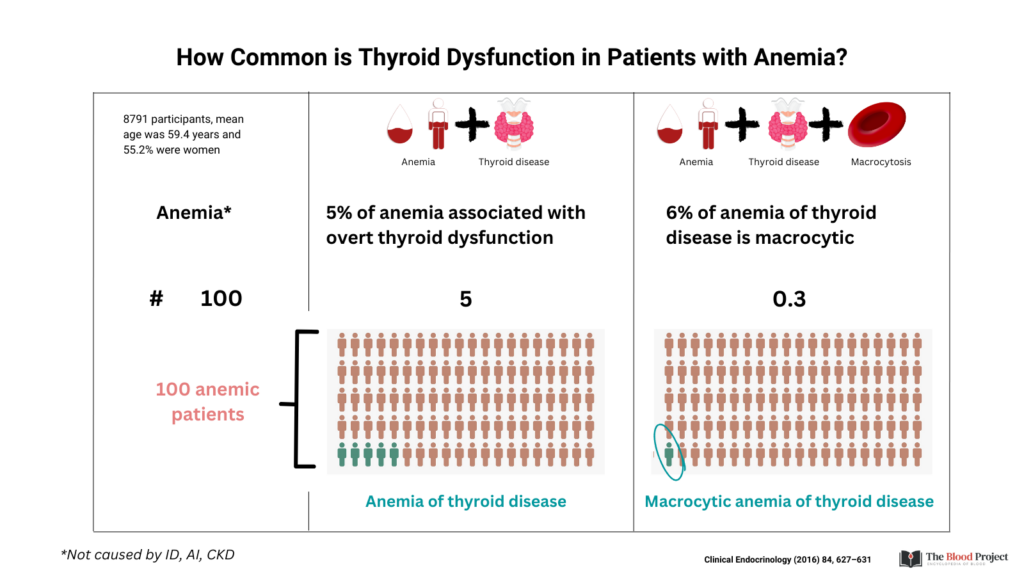
Study #1
- 8791 participants
- Median age 59.4 y
- 55.2% women
- Findings:
- 4.8% had overt thyroid dysfunction (either hypothyroidism or hyperthyroidism), after excluding those with iron deficiency, anemia of inflammation and CKD
- 0.3% had macrocytic anemia
Study #2
- 628 patients
- Median age 68
- 40% female
- 1.1% had evidence of hypothyroidism

Study #3
- Randomized, double-blind, placebo-controlled parallel group trials on levothyroxine treatment for subclinical hypothyroidism
- 669 participants had Hb levels measured at baseline:
- 337 allocated to placebo group
- 332 allocated to levothyroxine group
- Median age of 75 years (range, 65-97)
- Findings:
- No association was observed between TSH or fT4 levels and hemoglobin levels in univariable and multivariable regression models
- Higher levels of TSH or fT4 were not associated with increased odds of having anemia
- Median hemoglobin levels at baseline were comparable across quartiles of TSH and fT4
- Although significant reductions in TSH and increases in fT4 over 12 months of follow-up were observed in the levothyroxine group compared with the placebo group, no differences between the groups were observed in the change in hemoglobin levels after 12 months of follow-up
- No difference in change of hemoglobin levels after 12 months was identified in 69 participants with anemia at baseline
- Levothyroxine treatment was not associated with decreased odds of developing anemia (placebo n = 17/272, levothyroxine n = 19/277, OR 1.16 [95% CI, 0.59 to 2.29], P = 0.675) or increased odds of resolution of anemia

Bottom line:
Thyroid dysfunction is a rare cause of anemia (about 5% of cases) and an even rarer cause of macrocytic anemia (about 1% of cases). Even if hypothyroidism is diagnosed in a patient with anemia, achievement of a euthyroid state with levothyroxine treatment does not reverse the anemia or prevent development of anemia, casting doubt on a causal role. So, ordering a TSH in a patient with anemia has low yield, and the finding of an elevated TSH does not predict for response to treatment.
B) Now let’s look at the data from the thyroid dysfunction –> anemia angle
Study #1
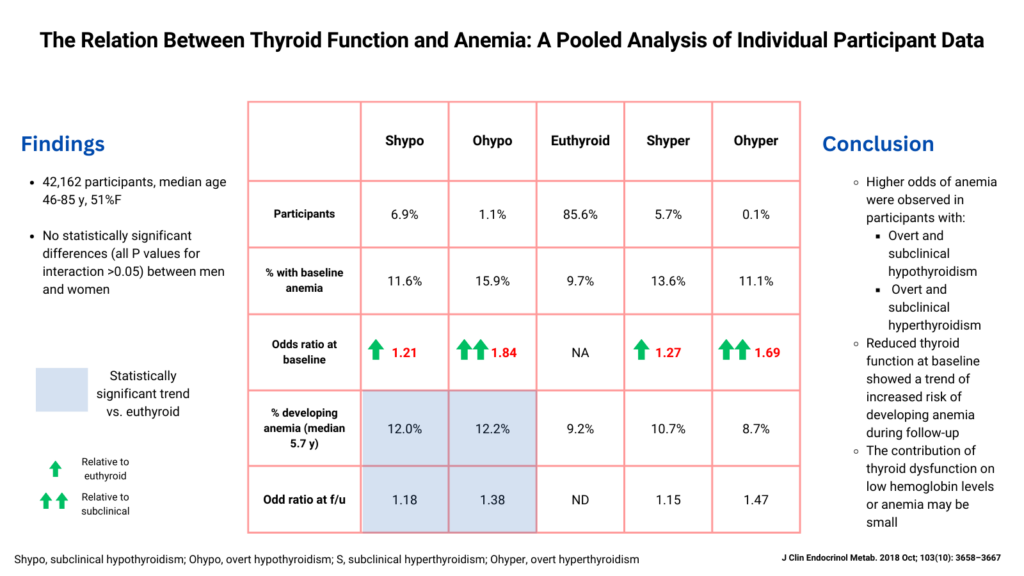
- 42,162 participants
- Median age 46-85 y in different cohorts
- 51% female
- Findings
- Higher odds of anemia were observed in participants with:
- Overt and subclinical hypothyroidism
- Overt and subclinical hyperthyroidism
- Reduced thyroid function at baseline showed a trend of increased risk of developing anemia during follow-up
- The contribution of thyroid dysfunction on low hemoglobin levels or anemia was small
- Higher odds of anemia were observed in participants with:
Study 2
- 12,337 participants
- Findings:
- No relevant differences were observed in Hb concentration among TSH categories
- No relevant association was found between fT4 and anemia
- In multivariable analyses, Hb was 0.22 g/dL lower in OHypo than in euthyroidism, and 0.08 g/dL lower in OHyper. No association was found in SHypo/SHyper
- Subclinical thyroid dysfunction was not associated with
- Baseline anemia
- Development of developing anemia
- A change in Hb concentration during follow-up
- OHypo and OHyper:
- Associated with anemia in the cross-sectional analyses

Study 3
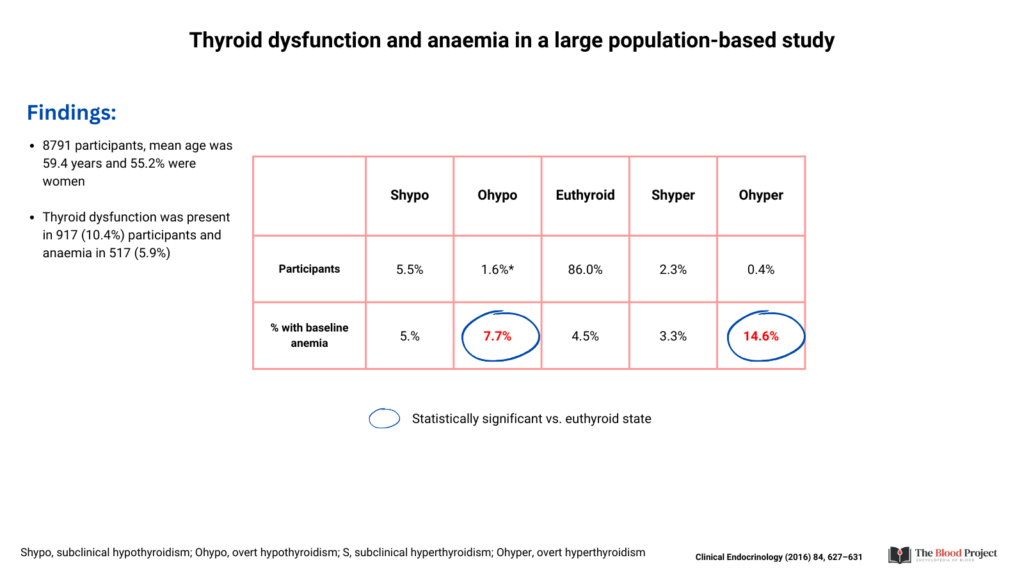
- 8791 participants
- Mean age 59.4 y
- 55.2% were women
- Thyroid dysfunction was present in 917 (10.4%) participants and anaemia in 517 (5.9%)
Bottom line:
There is some signal that thyroid dysfunction (especially overt hypo/hyperthyroidism in two studies and hypothyroidism in one study) is associated with a small, but significant increased risk of anemia (at baseline and/or over time). But as hematologists, we are referred patients with anemia, not with thyroid disorders, so as much as the potential association is interesting, we should take note of the extremely low prevalence of thyroid disease in patients with anemia.