Why hemoglobin does not fully capture the disease
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
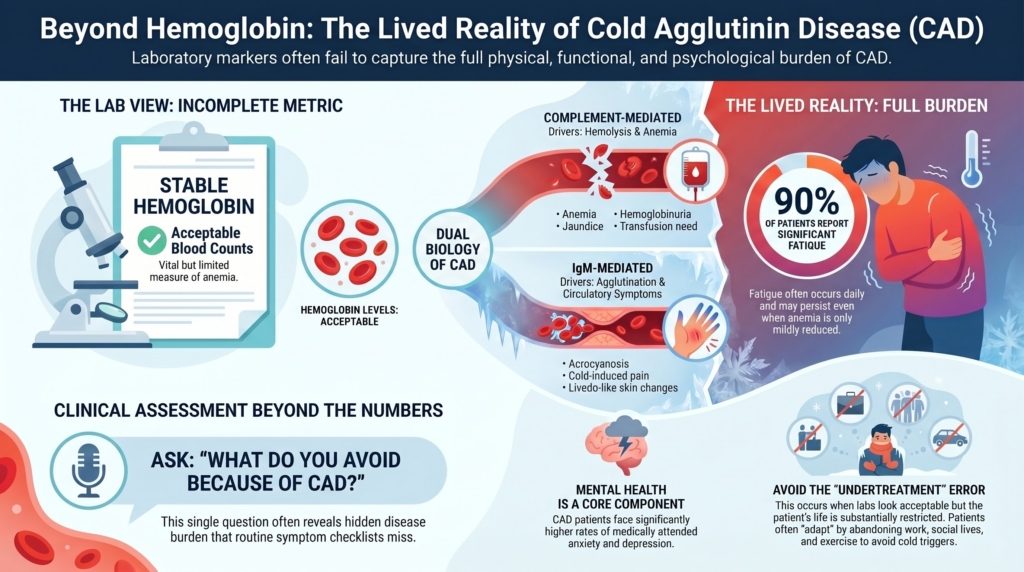
Cold agglutinin disease is often described through hemoglobin values, hemolysis markers, antibody titers, and complement activation. Those measures are essential. They are not enough.
CAD can impose a burden that is only partly visible in the laboratory. Fatigue, cold sensitivity, acrocyanosis, Raynaud-like symptoms, dyspnea, lifestyle restriction, transfusion dependence, health care use, anxiety, and treatment burden may shape daily life as much as the hemoglobin concentration itself.1
The central point is this:
CAD burden is not measured by hemoglobin alone.
This spoke focuses on the lived disease: what patients experience, why symptoms may diverge from laboratory severity, and how quality-of-life burden should inform treatment decisions.
The burden hemoglobin misses
Hemoglobin is a useful measure of anemia. It is not a complete measure of disease.
Two patients with the same hemoglobin may have very different lives. One may function well with stable compensated hemolysis. Another may experience disabling fatigue, cold-induced pain, dyspnea, activity restriction, or recurrent exacerbations.
This mismatch reflects the dual biology of CAD:
- complement-mediated hemolysis, which contributes to anemia, jaundice, fatigue, dyspnea, hemoglobinuria, transfusion need, and exacerbations
- IgM-mediated red-cell agglutination, which contributes to acrocyanosis, Raynaud-like symptoms, cold-induced pain or numbness, livedo-like skin changes, and microvascular flow disturbance
These mechanisms overlap, but they are not identical. Complement inhibition can improve hemolysis, hemoglobin, and fatigue by blocking the classical complement pathway downstream of IgM binding. It does not remove the IgM-producing clone, and it does not prevent IgM from binding red cells in cooler vascular beds. This explains a central clinical dissociation in CAD: hemolysis can improve while cold-induced circulatory symptoms persist.2
Fatigue is central to the patient experience
Fatigue is one of the most common and important symptoms in CAD.
In the development of the CAD-Symptoms and Impact Questionnaire, reactions to cold environments and fatigue were each reported by 93.8% of participants in concept elicitation interviews. In a separate web-based survey of 50 American patients, 90% reported fatigue, and many reported that fatigue occurred daily or several times per week.3
Fatigue may reflect anemia, but it may also reflect chronic hemolysis, complement activation, inflammation, sleep disruption, comorbidity, or the psychological burden of living with a fluctuating disease. The causal mix differs from patient to patient, but the clinical implication is consistent: fatigue should not be dismissed simply because hemoglobin is only mildly reduced.
Patients may be told that their anemia is “not severe enough” to explain their symptoms, even when the disease is meaningfully impairing function.
Fatigue should therefore be assessed directly:
- What activities has the patient stopped doing?
- Has work, exercise, travel, or social life changed?
- Does fatigue fluctuate with cold exposure, infection, or hemolysis?
- Is the patient recovering normally after exertion?
- Does the patient feel safe planning normal activities?
A stable hemoglobin does not guarantee a stable life.
Cold sensitivity and behavioral burden
Cold avoidance is a rational supportive strategy. It can also become a major life restriction.
Patients may avoid winter activities, air-conditioned spaces, grocery freezer aisles, swimming, travel, outdoor work, or ordinary tasks such as handling cold food. Some patients dress defensively, plan routes around temperature exposure, or carry gloves and warming devices year-round.
In the CAD-SIQ development study, reactions to cold environments were among the most frequently reported symptoms, and the final 11-item instrument included cold sensitivity, wearing extra clothing, limited physical, social, and enjoyable activities, difficulty with usual activities, mood, frustration, and anxiety or stress.4
In the web-based patient survey, CAD was reported to affect physical well-being, emotional well-being, social life, and household finances.5
These observations matter because CAD burden can become invisible when patients adapt. A patient may stop gardening, avoid family events in cold weather, decline travel, give up winter walks, change shopping habits, or rearrange work around temperature exposure, then describe symptoms as “manageable.”
The clinician’s task is not only to ask whether symptoms occur. It is to ask what life has become in order to keep symptoms from occurring.
A useful clinic question is:
“What do you avoid because of CAD?”
That question often reveals disease burden that routine symptom checklists miss.
Circulatory symptoms may matter even when anemia is modest
Cold-induced circulatory symptoms can include:
- acrocyanosis
- Raynaud-like color change
- cold-induced pain or numbness
- other cold-induced skin changes, including livedo-like patterns
- impaired manual function in cold conditions
- rare severe ischemic complications
These symptoms reflect agglutination and impaired microvascular flow in cooled vascular beds. They may not track closely with hemoglobin, bilirubin, LDH, or haptoglobin.
This is one reason CAD treatment decisions should not be driven by anemia alone. In some patients, the dominant burden is not low hemoglobin but loss of function, pain, or fear of cold exposure. Atypical or prominent vascular skin findings should also prompt consideration of other cold-sensitive disorders, including cryoglobulinemia when clinically appropriate.6
CAD fluctuates over time
Patients often describe CAD as variable rather than constant.
In a web-based survey, 88% of respondents reported previous episodes of increased intensity or sensitivity of CAD symptoms, and 42% reported that their symptoms had worsened since diagnosis. Common triggers included cold temperature, winter, and air conditioning.7
CAD can also worsen with cold exposure, infection, trauma, surgery, or physiologic stress. Even when patients are stable, they may live with concern about the next flare.8
This fluctuation creates practical and emotional burden. Patients may feel well enough at one visit but remain uncertain about the next infection, cold exposure, weather change, transfusion, or hospitalization.
Unpredictability itself becomes part of the disease.
Mental health belongs in the clinical landscape
CAD is not only physically restrictive. It can also affect emotional health.
A claims-clinical analysis found that patients with CAD had a higher rate of medically attended anxiety and depression than matched non-CAD comparators, with increased risk also seen in analyses restricted to primary CAD.9
This does not mean every patient with CAD has anxiety or depression. It does mean that mental health burden belongs in the clinical landscape, not outside it. Fear of exacerbation, concern about cold exposure, repeated health care visits, and uncertainty about treatment duration can all shape quality of life.
Mental health burden should therefore be recognized, asked about, and addressed when present.
CAD also creates health care burden
CAD burden is not limited to symptoms.
Real-world analyses show substantial health care use, including outpatient visits, transfusions, emergency department visits, hospitalizations, and multiple lines of therapy. In a Stanford longitudinal cohort, most patients had moderate or severe anemia at disease onset, many experienced severe anemia events over time, and at least 65% received transfusions during the disease course. In a larger Optum electronic health record analysis, moderate or severe anemia and hemolysis persisted over follow-up, and health care resource use was generally greater among patients with severe anemia.10
For patients, this translates into time, logistics, worry, cost, and disruption.
A disease can be “rare” and still occupy a large amount of a patient’s life.
Treatment burden also affects quality of life
Treatment can reduce disease burden. It can also create burden.
Complement-directed therapy may offer rapid control of hemolysis, but usually requires ongoing infusions and does not target the IgM-producing B-cell clone or cold agglutinin production. Clone-directed therapy may offer longer treatment-free intervals, but involves delayed response, immunosuppression, cytotoxicity in some regimens, and risk of infection. Supportive management may avoid drug toxicity but may leave symptoms or restrictions in place.11
Treatment burden includes:
- infusion schedule
- travel time
- laboratory monitoring
- adverse effects
- infection precautions
- financial or access barriers
- anxiety about relapse after stopping therapy
- uncertainty about duration of treatment
A treatment can be biologically effective and still poorly aligned with a patient’s life. Conversely, a less intensive strategy may be reasonable when burden is low and disease trajectory is stable.
Patient-reported outcomes matter
Clinical trials in CAD increasingly include fatigue and patient-reported outcome measures, not just hemoglobin and hemolysis markers.
In CADENZA, sutimlimab improved patient-reported outcomes compared with placebo, including clinically meaningful improvement in FACIT-Fatigue beginning early in treatment and sustained through the 26-week treatment period. The least-squares mean change in FACIT-Fatigue score from baseline to the treatment assessment timepoint was 10.8 points with sutimlimab versus 1.9 points with placebo. The study also evaluated broader measures including SF-12, EQ-VAS, Patient Global Impression of Change, and Patient Global Impression of fatigue Severity.12
Longer-term CARDINAL follow-up showed sustained improvements in patient-reported outcomes over 2 years of ongoing sutimlimab therapy, with FACIT-Fatigue improvement remaining above a clinically important change during treatment and returning toward baseline after treatment cessation.13
This reflects an important shift: treatment success is not only biochemical control. It is also improvement in how patients feel and function.
When quality of life contributes to treatment decisions
Treatment is generally considered when CAD causes clinically meaningful harm. Quality-of-life burden is one way that harm becomes visible.
Quality-of-life burden may contribute to the decision to treat when it is attributable to CAD and clinically substantial, especially when patients experience:
- fatigue that limits work, caregiving, exercise, or social life
- recurrent or severe cold-induced circulatory symptoms
- transfusion need or repeated urgent visits
- inability to tolerate routine cold exposure despite precautions
- recurrent exacerbations
- persistent behavioral restriction caused by disease unpredictability
- mental health burden that appears linked to CAD-related uncertainty, restriction, or recurrent flares
- a mismatch between “acceptable” laboratory values and unacceptable lived burden
The key question is not simply:
How low is the hemoglobin?
The better question is:
How much of this patient’s life is being organized around CAD?
How to ask about CAD burden in clinic
Clinicians often ask about symptoms. CAD requires asking about adaptation.
Useful questions include:
- What do you avoid because of cold sensitivity?
- How has CAD changed your work, exercise, travel, or social life?
- Do you plan your day around temperature exposure?
- How often do you experience fatigue that limits activity?
- Are you afraid of infection, cold weather, or procedures because of prior exacerbations?
- Do symptoms improve, worsen, or persist despite treatment?
- Which bothers you more: anemia-related symptoms, cold-induced symptoms, or treatment burden?
- What outcome would make treatment worthwhile to you?
These questions help identify the dominant burden: hemolysis, agglutination symptoms, treatment burden, uncertainty, or some combination.
Clinical practice note: aligning treatment with burden
Quality-of-life assessment helps determine which therapeutic question matters most.
| Dominant burden | Likely clinical question | Strategy to consider |
|---|---|---|
| Stable mild anemia, minimal symptoms | can we observe safely? | observation and supportive management |
| Active hemolysis, worsening anemia, transfusion need | can we control hemolysis now? | complement-directed therapy, transfusion support when needed |
| Persistent IgM-mediated circulatory symptoms | can we reduce pathogenic antibody production? | clone-directed therapy or strategies aimed at the antibody source |
| High burden from continuous therapy | can we reduce treatment dependence? | reassessment, possible clone-directed strategy, shared decision-making |
| Fluctuating symptoms with unclear driver | what mechanism is dominant? | reassess hemolysis, agglutination symptoms, clone, triggers, and comorbidities |
This table is not an algorithm. It is a way to make the patient’s burden visible and connect it to mechanism.
Evidence anchor: patient-reported and real-world burden in CAD
| Evidence source | What it adds | Key message |
|---|---|---|
| CAD-SIQ development study | qualitative interviews and development of a CAD-specific patient-reported outcome instrument | fatigue, cold sensitivity, dyspnea, activity limitation, mood, frustration, and anxiety/stress are central patient-reported concepts14 |
| Web-based patient survey | patient-reported daily-life burden among 50 American patients | fatigue was common, symptoms fluctuated, and CAD affected physical, emotional, social, and financial domains15 |
| Stanford longitudinal cohort | anemia severity, transfusion burden, therapies, and health care use over time | severe anemia events and transfusion exposure were frequent in a tertiary-care cohort16 |
| Optum EHR burden analysis | large real-world cohort with longitudinal anemia, hemolysis, therapy, transfusion, and health care resource utilization data | CAD imposed substantial long-term burden on patients and health systems, especially with severe anemia17 |
| CADENZA PRO analysis | randomized placebo-controlled evidence for patient-reported benefit with sutimlimab | complement inhibition improved fatigue and broader patient-reported outcomes in CAD without recent transfusion18 |
| CARDINAL long-term PRO analysis | longer-term patient-reported outcomes with continued sutimlimab | quality-of-life benefits were sustained during treatment and returned toward baseline after cessation19 |
| Anxiety/depression analysis | matched claims-clinical analysis of medically attended mental health burden | CAD was associated with increased medically attended anxiety and depression compared with matched controls20 |
Avoiding two errors
Quality-of-life assessment helps avoid two opposite mistakes.
Undertreatment occurs when laboratory values look acceptable but the patient’s life is substantially restricted.
Overtreatment occurs when laboratory abnormalities are treated despite low burden, stable trajectory, or patient preference for observation.
Both errors arise when clinicians focus on numbers without asking how the disease is functioning in the patient’s life.
Clinical synthesis
CAD is a disease of blood, complement, temperature, and clone. It is also a disease of adaptation.
Patients may change how they dress, travel, work, exercise, shop, plan, and seek care. Some restrictions are obvious. Others become invisible because the patient has already reorganized life around them.
Quality-of-life burden should not replace laboratory assessment, but it should change how laboratory results are interpreted. Hemoglobin, bilirubin, LDH, cold agglutinin titer, and thermal amplitude describe important parts of the disease. The patient’s lived experience describes another.
Expert care requires both.
Key takeaways
- hemoglobin is incomplete: anemia severity does not fully capture CAD burden.
- fatigue matters: fatigue is common, often functionally limiting, and should be assessed directly.
- cold avoidance has a cost: fewer cold-induced episodes may reflect lifestyle restriction, not absence of disease.
- symptoms have different mechanisms: hemolysis and circulatory symptoms may respond differently to therapy.
- mental health is part of burden: anxiety, depression, and fear of exacerbation may shape quality of life.
- treatment burden counts: continuous therapy, immunosuppression, monitoring, and access can shape quality of life.
- patient-reported burden is clinical data: lived experience should be interpreted alongside mechanism and laboratory findings.
- the goal is alignment: treatment should fit disease biology, trajectory, and the patient’s life.
Reflect and Apply
Think of a patient with CAD whose hemoglobin seemed “acceptable.”
Pause and ask:
What parts of life had the patient changed because of CAD?
Were symptoms driven mainly by hemolysis, cold-induced agglutination, treatment burden, or uncertainty?
Did the management plan address the patient’s lived burden, or only the laboratory pattern?
The goal is not to treat every symptom. The goal is to understand which burdens are disease-related, which are modifiable, and which matter most to the patient.
Test your thinking
A short, judgment-focused quiz on quality of life and disease burden in cold agglutinin disease.