Aligning treatment with what matters to the patient
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
Cold agglutinin disease is not a one-decision illness. The core hemolytic mechanism is well characterized, but treatment thresholds are not determined by hemoglobin alone.
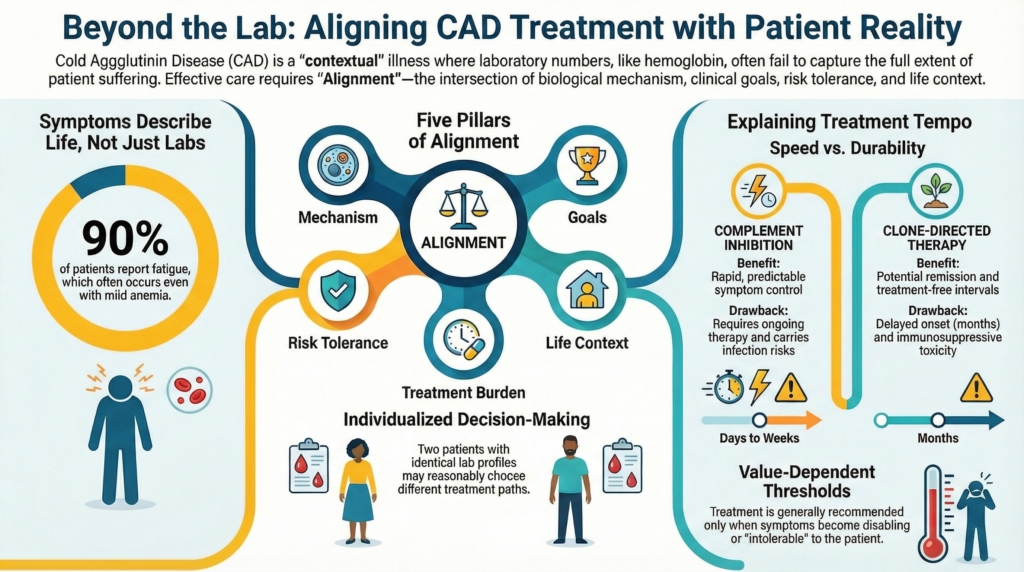
Even when biology is well defined and therapeutic options are established, optimal management depends on how decisions are aligned with a patient’s values, priorities, risk tolerance, and lived experience. Two patients with identical laboratory profiles may reasonably choose different paths.
Together with Treatment Strategy and Sequencing, this framework defines how CAD is managed: the question, the timing, and the alignment.
Expert CAD care integrates biological precision with individualized decision-making.1
Patient-centered care in CAD is not about preference replacing evidence.
It is about evidence being applied in a way that fits the person living with the disease.
Alignment is the governing concept.
Alignment is the intersection of:
- mechanism
- clinical goals
- risk tolerance
- life context
- treatment burden
Treatment decisions are strongest when these variables point in the same direction.
CAD decisions involve trade-offs, not right answers
Most disease-directed decisions in CAD involve real trade-offs:
- rapid control versus long-term modification
- continuous therapy versus finite treatment
- predictability versus uncertainty
- symptom relief versus treatment burden
- disease control versus treatment risk
In CAD these are not abstractions. They map directly onto therapeutic strategy:
- complement inhibition prioritizes speed and predictability
- clone-directed therapy prioritizes durability and treatment-free intervals
Principle
These trade-offs cannot be resolved by guidelines alone.
They require shared deliberation.
What patients are often deciding between
From a patient perspective, CAD decisions are rarely framed as‘Which drug is best’?
They are more often framed as:
- Do I want fast, reliable control even if it means ongoing therapy?
- Am I willing to accept delayed benefit and immunosuppression for the possibility of remission?
- How much treatment burden is acceptable for my current symptoms?
- What level of anemia or cold sensitivity is tolerable to me?
- How do treatment choices fit into work, travel, caregiving, or climate exposure?
Expert clinicians make these implicit questions explicit.
Treatment is generally recommended only when anemia is symptomatic, transfusion-dependent, or accompanied by disabling circulatory symptoms, meaning that the very decision whether to treat is already value-dependent.2
Symptom burden matters independently of hemoglobin
Patients experience CAD through symptoms, not numbers.
Key realities:
- fatigue, cold-induced pain, and acrocyanosis may dominate quality of life
- symptom severity often correlates poorly with hemoglobin
- patients may feel impaired despite “acceptable” labs
- others function well despite severe anemia
This is one of the most common forms of misalignment: numbers and lived experience pointing in different directions.
In survey data, approximately 90% of patients report fatigue, and this symptom may be prominent even when anemia is mild.3
This dissociation suggests that hemoglobin alone does not capture total disease burden, which may also reflect circulatory manifestations of the disease.
Quality-of-life studies across autoimmune hemolytic anemias confirm substantial impairment in daily functioning, sleep, and work participation.4
Patient-centered care therefore requires:
- direct inquiry into functional impact
- avoidance of rigid numeric thresholds
- validation of symptoms that are biologically real but numerically subtle
Treating CAD based solely on hemoglobin risks undertreating suffering or overtreating stability.
Numbers describe physiology.
Symptoms describe life.
Risk tolerance varies, and in CAD it has structure
Risk tolerance is not random variation. In CAD it often reflects how patients weigh specific therapeutic realities:
- complement inhibition offers rapid control but requires ongoing therapy and carries infection risk
- clone-directed therapy offers potential remission but has delayed onset and immunosuppressive toxicity
Some patients prioritize immediacy and predictability.
Others prioritize durability and independence from therapy.
There is no correct risk tolerance.
There is only informed risk tolerance.
Treatment selection in autoimmune hemolytic anemia, including CAD, is influenced by patient preference, clinician experience, and drug availability, reflecting the inherently individualized nature of decision-making.5
Variation is not a barrier to good care.
It is the reason shared decision-making exists.
Explaining tempo is part of informed consent
Time is a therapeutic variable in CAD.
Patients need to understand:
- which therapies act within days to weeks
- which act over months
- what early response looks like
- when patience is appropriate
- when lack of improvement signals strategy failure
Rituximab-based therapy may require months for response, and this delay must be anticipated when choosing treatment sequences.6
Conversely, complement inhibition produces rapid control but does not modify the underlying clone, meaning speed and durability often sit on opposite ends of the decision spectrum.
Misaligned expectations about tempo are a common source of mistrust.
Clear framing prevents:
- abandoning effective therapy too early
- persisting with ineffective therapy too long
Understanding time is not a courtesy.
It is part of informed consent.
Reassessment is a shared process
CAD is heterogeneous and fluctuating, so reassessment is expected, not corrective.7
Reassessment is not something done to patients.
It is something done with them.
Shared reassessment includes:
- reviewing symptom trajectory, not just labs
- revisiting whether goals have shifted
- acknowledging when burden outweighs benefit
- adjusting strategy without framing prior decisions as mistakes
Patients contribute information no laboratory can supply: how treatment affects energy, work, cognition, cold tolerance, and daily life. Without that input, reassessment is incomplete.
When patients decline recommended therapy
Some patients decline disease-directed treatment despite clinical indication.
This is not a failure of care.
It is a decision point.
Patient-centered management in this setting includes:
- ensuring understanding of risks and alternatives
- optimizing supportive measures
- documenting goals clearly
- maintaining open pathways for reconsideration
- avoiding coercive framing
In CAD specifically, decisions often change as disease tempo changes. A patient who declines therapy during stability may reconsider during exacerbation. Planning for that possibility preserves alliance and safety simultaneously.
Respecting autonomy does not require abandoning vigilance.
Communication is itself therapeutic
How CAD is explained shapes how it is lived.
Helpful framing includes:
- emphasizing control rather than cure
- distinguishing dangerous disease from disruptive disease
- normalizing fluctuation
- acknowledging uncertainty without minimizing seriousness
Example language that accomplishes this balance:
“Your disease is real and biologically active, but it is also manageable. Our goal is not to eliminate it overnight. Our goal is to control it safely in a way that fits your life.”
Communication reduces distress even when biology cannot be eliminated.
Explicit principle
Patient-centered decision-making in cold agglutinin disease does not weaken clinical rigor.
It completes it.
Expert care matches mechanism to moment and treatment to the person.
The best decision is not the same as the most aggressive one.
Success is defined not only by laboratory targets, but by how safely and fully a patient is able to live with their disease.
The best decision is the one that fits the person, not the one that looks ideal on paper.
Reflect and Apply
Think of a patient with CAD whose laboratory profile suggests treatment may be reasonable.
Before choosing a strategy, ask:
What is the patient actually trying to regain?
Energy, warmth, independence, fewer transfusions, safer travel, less fear of cold exposure, or freedom from ongoing therapy?
What trade-off are they most willing to accept?
Speed versus durability, continuous therapy versus finite treatment, symptom control versus treatment burden, or certainty versus risk?
In patient-centered CAD care, the question is not only:
What treatment fits the disease?
It is also:
What treatment fits this person’s life?
Test your thinking
A short, judgment-focused quiz on patient-centered decision making in cold agglutinin disease.