Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
House staff are often taught two competing slogans:
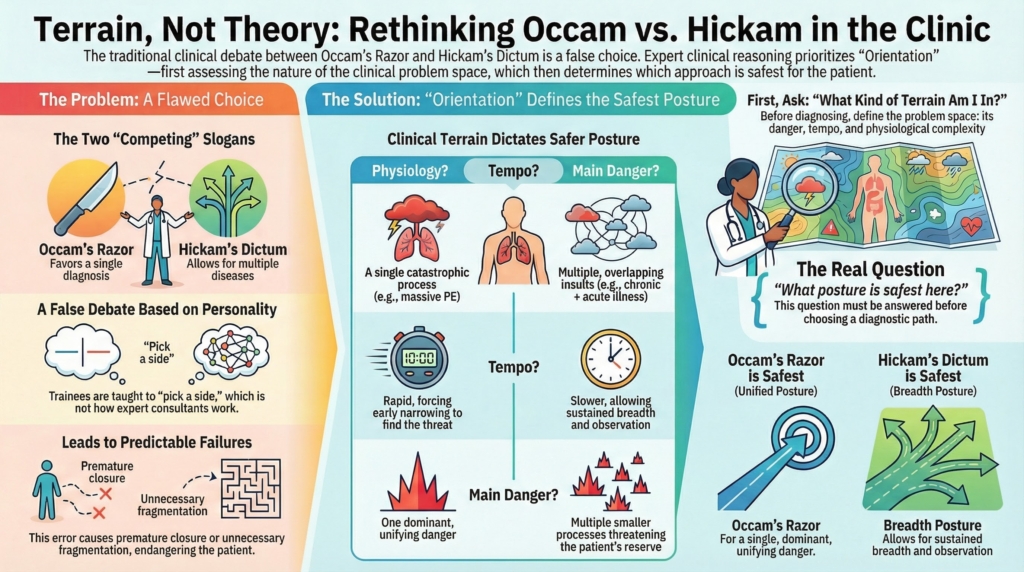
- Occam’s razor: favor a single unifying diagnosis
- Hickam’s dictum: patients can have as many diseases as they want
These are usually presented as philosophical preferences or stylistic differences in clinical reasoning.
In real consult work, that framing is misleading.
Consultants are rarely choosing between Occam and Hickam as abstract principles. They are deciding something more fundamental first:
What kind of clinical world am I in right now?
That is an Orientation task, not a Thinking preference.
Occam’s razor and Hickam’s dictum are not upstream rules.
They are downstream expressions of terrain.
The false debate
When Occam and Hickam are taught as opposing schools of thought, trainees are left with a false choice:
- Should I be parsimonious?
- Or should I assume multiple problems?
This turns clinical reasoning into a personality trait:
- “I’m more of an Occam person.”
- “I lean Hickam.”
That is not how expert consultants actually work.
In practice, neither principle is inherently right or wrong.
What matters is whether the clinical terrain makes unification safe — or whether breadth is required to protect the patient.
That determination happens before diagnosis.
It happens in Orientation.
What consultants are really deciding
Before choosing whether to unify or separate problems, consultants implicitly define:
- how dangerous the terrain is
- how much uncertainty is tolerable
- whether physiology is likely unified or fragmented
- whether tempo favors early narrowing or prolonged breadth
- whether reserve-threat is present
- whether deterioration could be hidden or rapid
These are not diagnostic questions.
They are problem-space questions.
They define the kind of clinical world the diagnosis will have to live in.
Only after that world is defined does Occam or Hickam become relevant.
Orientation determines whether Occam is safe
Occam’s razor is safest when the terrain supports unification.
Examples include:
- a single catastrophic physiology (e.g., TTP, massive PE, acute leukemia)
- a tightly coupled pathophysiologic process
- rapid tempo with a dominant unifying danger
- situations where delay in unification increases harm
In these terrains, breadth can be dangerous.
Failure to unify early may miss the central threat.
Here, Orientation narrows the terrain.
Thinking then assigns weight within that narrowed world.
Execution makes early escalation visible.
Occam is not a philosophy here.
It is a posture earned by terrain.
Orientation determines when Hickam is safer
Hickam’s dictum is safest when the terrain supports overlap.
Examples include:
- hospitalized patients with multiple insults
- mixed medication effects
- nutritional, infectious, and inflammatory physiology coexisting
- chronic disease layered on acute illness
- reserve-threat states where multiple small processes matter
In these terrains, forced unification is dangerous.
The patient is not in a single-disease world.
They are in a multi-process world.
Here, Orientation broadens the terrain.
Thinking assigns provisional weight across categories.
Execution maintains vigilance and avoids premature closure.
Hickam is not philosophical generosity.
It is protective posture.
Why this is an Orientation problem, not a Thinking preference
Occam and Hickam are often taught as reasoning styles.
That’s a category error.
They are not primarily about how you think.
They are about what kind of problem you believe you are in.
That belief is established in Orientation.
Orientation answers:
- Is this likely unified or fragmented physiology?
- Is there one dominant danger or several moderate ones?
- Is tempo forcing early narrowing or sustained breadth?
- How much uncertainty can this patient tolerate safely?
Only after those questions are answered does Thinking properly assign weight.
Without Orientation, Occam and Hickam become slogans.
With Orientation, they become context-dependent tools.
The teaching error
A common teaching error is to present Occam and Hickam without teaching problem-space definition.
This trains the wrong instinct.
Trainees learn to debate:
- “Is this Occam or Hickam?”
Instead of asking:
- “What kind of terrain am I in?”
This leads to two predictable failures:
- premature unification in mixed physiology
- unnecessary fragmentation in unified catastrophic states
Both are posture errors, not knowledge errors.
How Execution makes the posture visible
In expert consults, this posture is made explicit through language.
Occam posture sounds like:
- “This looks like a single unifying physiology that explains the pattern. We should treat this as one process until proven otherwise.”
Hickam posture sounds like:
- “This likely represents overlapping processes. We should hold multiple contributors in parallel and let trajectory clarify.”
These are not diagnostic statements.
They are terrain declarations.
They align the team’s uncertainty tolerance and vigilance.
That is Execution making Orientation visible.
Reframing the slogans
A more accurate teaching reframing would be:
- Occam’s razor is safest in unified, time-sensitive terrains
- Hickam’s dictum is safest in mixed, reserve-threat terrains
You don’t choose between them.
Orientation chooses for you.
Bottom line
Occam’s razor and Hickam’s dictum are not competing philosophies.
They are downstream expressions of terrain.
Orientation defines what kind of clinical world you are in.
Thinking assigns weight within that world.
Execution makes that posture visible to others.
If Orientation is wrong, even elegant reasoning will occur in the wrong terrain.
In Consult Practice, the real question is not:
- “Is this Occam or Hickam?”
It is:
“What kind of problem space am I in right now — and what posture is safest here?”
That question comes first.