Bottom line
- Obesity is associated with an elevated white blood cell (WBC) count, primarily neutrophils (but also lymphocytes).
- The WBC count is usually elevated within the normal range, but can exceed the upper limit of normal, leading to leukocytosis.
- Obesity-associated leukocytosis is believed to be caused by cytokines that are released from adipose tissue and lead to demargination of circulating neutrophils, and increased production and release of neutrophils from the bone marrow.
- There are some studies showing that this trend can be reversed with bariatric surgery, providing evidence for a cause-effect relationship between obesity and WBC count.
- It seems reasonable to ascribe a (slightly) elevated count to obesity in an otherwise healthy patient without conducting an extensive work up.
Introduction
- Obesity is associated with low grade systemic inflammation characterized by an adipose tissue driven acute-phase response that promotes interleukin (IL)-6, IL-1, IL-8, and tumor necrosis factor (TNF)-α mediated induction of acute-phase proteins such as C-reactive protein (CRP).1
- Obesity is associated with an increase in WBC count and absolute neutrophil count, usually within the normal range, but occasionally leading to leukocytosis.
- The effect of obesity on the WBC count is greater in women compared to men.
- Bariatric surgery results in amelioration of the elevated WBC count.2
Definitions
- Obesity is usually defined as body mass index (BMI) ≥ 30 kg/m2:
- BMI defined as weight in kilograms divided by square of height in meters, or use BMI calculator.
- Overweight defined as BMI 25-29.9 kg/m2.
- Obesity typically categorized into 3 classes.
- Leukocytosis in a non-pregnant adult is defined by a white cell count > 11 x 109/L.
Epidemiology
- Most epidemiological studies have shown that while obese subjects have higher white blood counts than lean individuals, the absolute leukocyte count of obese subjects is generally within the normal range.3
- However, it is not uncommon for patients to be referred to a hematologist for evaluation of unexplained leukocytosis, who are obese and yet whose extensive work-up is otherwise negative.
- “A significant number of patients referred for investigation of unexplained leukocytosis have no identifiable cause of a persistent and stable leukocytosis, other than their being obese.”45
- The actual percentage of obese patients who have leukocytosis and the number of patients with leukocytosis explained by obesity is poorly defined and varies widely between studies (see cohort studies below).
Pathophysiology
- Adipose tissue is a primary source of inflammatory mediators.6
- Adipose tissue is composed of:7
- Adipocytes
- Tissue macrophages:
- Comprise up to 40% of the cells in obese adipose tissue, compared with under 10% in lean individuals.
- Elevated macrophage infiltration is noted in visceral compared with subcutaneous fat.
- Most likely derived from bone marrow-derived circulating monocytes that subsequently infiltrated adipose tissue.
- Trafficking to adipose tissue may be mediated partly by leptin and other chemokines.
- Human adipose tissue (especially macrophages) produce and release cytokines and adipokines, which the induce the expression of acute-phase reactants (proteins), including:89
- IL-6
- IL-1
- IL-8
- TNF-α
- CRP:
- Elevation significantly corresponds to the level of adiposity present in the body.
- Decreases with weight loss.
- Pro-inflammatory cytokines such as IL-6and IL-8 are important inducers of leukocytosis, particularly neutrophilia, through multiple mechanisms including:10
- Demargination of circulating neutrophils.
- Acceleration of bone marrow neutrophil release.
- Enhancement of bone marrow granulopoiesis.
- Possible explanations for the greater effect of obesity on the WBC count in women compared to men include:11
- Higher levels of inflammatory mediators (eg, CRP) and leptin in women.
- Concomitant polycystic ovarian syndrome (PCOS).12
Clinical studies and cohorts
- Cohort studies:
- Fisch and Freedman, 1975:
- Data from 14,961 healthy women were analyzed to determine the relative importance of factors that alter the WBC count.
- The effects of smoking, oral contraceptive use, and obesity were most striking.
- A total leukocyte count greater than 10,000/cu mm was found in 44% of obese, heavily smoking women who took oral contraceptives (central 95% of the distribution was 5,800 to 14,200/cu mm) as compared to 2% of women without these attributes (3,500 to 9,400/cu mm).
- Other factors such as age, time of day, phase of the menstrual cycle, and red blood cell variables were of lesser significance.
- The use of non contraceptive estrogenic hormones did not affect the WBC count. Recognition of these findings is important because excessive laboratory studies, lost physician time, and patient inconvenience may thereby be avoided.
- Nanji el, 1985:
- 42 morbidly obese patients (weight range, 101.5-206.8 kg).
- None of the patients had a recent history of infection, hematologic disorders, chronic respiratory disease, or were smoking more than 5 cigarettes/day.
- Twelve of the 42 patients (29%) had a total leukocyte count of > 10 X 109 cells/L.
- There was no difference in the total leukocyte counts between the patients who were smokers (<5 cigarettes/day) and nonsmokers
- There was a significant correlation between body weight (kg) and total leukocyte count (r = 0.68, P less than 0.001).
- Authors’ conclusion: “Morbid obesity should be considered as one of the causes of physiologic leukocytosis.”
- Herishanu et al, 2006:
- n = 327 outpatients referred to hematology clinic for persistent leukocytosis:
- Causes included:
- Smoking in 29%
- Obesity in 15.3%
- Idiopathic (normal acute-phase reactant levels) in 12.5%
- Idiopathic-inflammatory (significantly elevated acute-phase reactants) in 9.2%
- Myeloproliferative disorders in 8%
- Smoking and obesity in 7.3%
- Lymphoproliferative diseases in 4.8%
- Inflammatory diseases in 2.7%
- Solid tumors in 2%
- Post splenectomy in 2%
- Causes included:
- Characteristics of the 15.3% of patients who were obese:
- Asymptomatic
- Mostly middle-aged females
- Mild leukocytosis (mean white blood cell count 13.05 ± 1.44 x 109/L) characterized mostly by neutrophilia without bandemia
- Elevated acute-phase reactants (CRP and erythrocyte sedimentation rate)
- There was no other recognized cause for the leukocytosis (for example, infection, inflammation, smoking, malignancy).
- During a mean follow-up of 45.6 months, the leukocytosis and the elevated acute-phase reactants persisted and no new causes for leukocytosis were evident.
- In a cross-sectional analysis of 3716 non-smoker subjects, 62 (1.2%) were found to have leukocytosis. Compared with the population with a normal white blood count range, these subjects with leukocytosis had higher BMI, serum C-reactive protein (CRP) levels, waist circumference, and neutrophil and platelet count (all P < 0.0005). After logistic regression analysis, only BMI was shown to be associated with leukocytosis (P < 0.0005).
- Authors’ conclusion: “Although the white blood counts are relatively high in obese subjects, the values are still within the normal range in most of the cases. The obese subjects associated with absolute leukocytosis and raised acute-phase reactants may in fact represent a subgroup of obese subjects characterized by more pronounced parameters of inflammation. The results of our cross-sectional study further support a relationship between obesity and leukocytosis. Recognition of the association between obesity and leukocytosis may have important clinical implications. We suggest that clinicians avoid unnecessary and extensive investigation of elevated white blood counts in obese subjects who have the features presented in this study.”
- n = 327 outpatients referred to hematology clinic for persistent leukocytosis:
- Charles et al, 2007
- Cross-sectional study among 104 randomly selected police officers (41 women and 63 men).
- Officers ranged in age from 26 to 61 years old and were predominantly white.
- Among women:
- Current smokers had significantly higher WBC counts (7.4 +/- 1.4) than former (5.2 +/- 1.4) or never smokers (5.6 +/- 1.5) (p = 0.002).
- Abdominal height was positively associated with platelet count after adjustment for depression (p for trend = 0.039).
- Women had similar WBC counts but higher mean platelet counts than men (p = 0.005).
- Among women and men, a non-significant step-wise trend was observed between abdominal height and mean WBC counts before and after adjustment for smoking, race, and physical activity.
- No association was observed between obesity and platelet count among men.
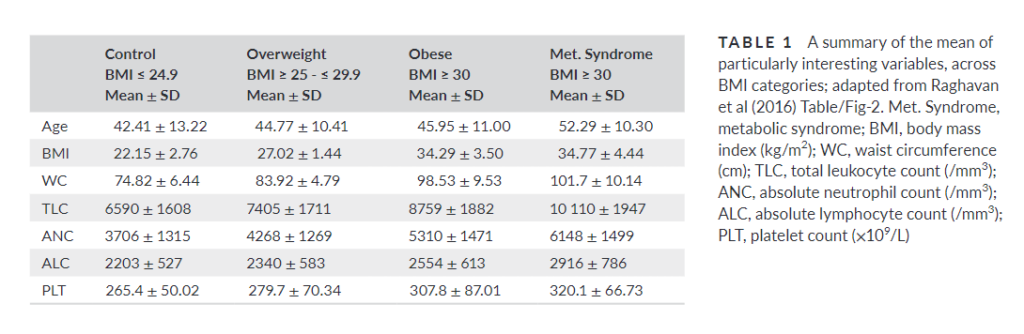
- Raghavan et, 2016:
- Case-control study of 243 female subjects allocated to four groups based on WHO and IDF criteria: Control, Overweight, Obese and Obese with Metabolic Syndrome.
- There was a strong positive correlation between obesity related anthropometric measurements (BMI, BF, WC) and leucocyte counts – TLC and ANC – which were statistically highly significant
- Leucocyte counts (TLC and ANC) showed strong positive correlation with:
- Obesity related anthropometric measurements (BMI, BF, WC)
- Fasting plasma glucose
- Mean values for TLC and ANC showed statistically significant difference between each and every group.
- The difference in the mean values of these parameters between obese and metabolic syndrome was highly significant.
- Fisch and Freedman, 1975:
- Cohort studies (cont’d):
- Julius et al, 2014:
- 391 individuals from the TRial Of Preventing HYpertension (TROPHY).
- Baseline BMI correlated with:
- WBC count (r = 0.185, P < 0.0001)
- Neutrophils (r = 0.135, P < 0.001)
- Lymphocytes (r = 0.204, P < 0.0001)
- Authors’ conclusion: “he significant independent association of WBCC with baseline BMI and triglycerides is consistent with the evidence that obesity and insulin resistance are associated with inflammation.”
- Chang and Lin, 2022:
- 720 nurses who had received health checkups at a large teaching hospital in Taiwan.
- WBC count was an independent factor relating to an overly large waist circumference or overly high body mass index (BMI) of nurses.
- For every 103/μL increase in WBC count, the risk of waist circumference exceeding 90 cm and 80 cm respectively in male and female nurses increased by 46%, and for every 103/μL increase in WBC count, the risk of a BMI 24 kg/m2 in nurses increased by 50%.
- Julius et al, 2014: