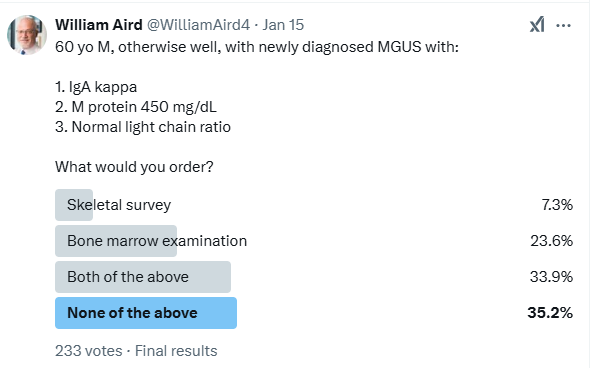
I posted a poll asking whether an otherwise well 60 yo M, who is newly diagnosed with monoclonal gammopathy of undetermined significance (MGUS) (IgA kappa M protein, M protein 450 mg/dL and a normal free light chain ratio) requires a skeletal survey and/or bone marrow aspirate and biopsy.
42.5% responded that they would not perform a bone marrow biopsy:
Some of the responders’ comments are shown below:
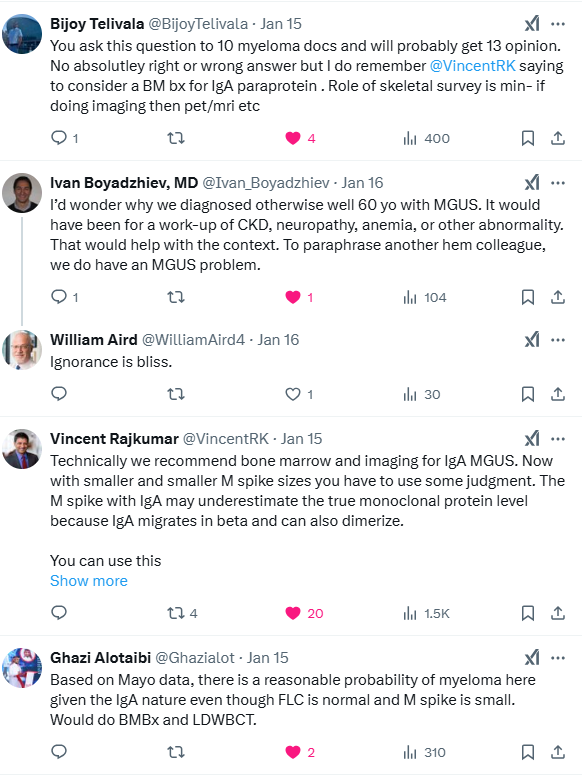
- Q: Why even consider a bone marrow examination in the first place?
- A: Because the bone marrow may upgrade the diagnosis to smoldering multiple myeloma (SMM; bone marrow plasma cells > 10%)) or [rarely] to multiple myeloma (MM) (plasma cells > 20%), both of which are potentially amenable to treatment
This tutorial focuses on the question of when to perform a bone marrow examination in a patient with MGUS. There is no right answer in this case (it depends on your assessment of the risks [pain, cost, inconvenience to the patient] vs. benefits [picking up SMM or MM, which are potentially treatable]), but let’s risk stratify the patient and then see how various experts and guideline organizations would recommend handling the question of bone marrow examination.
Let’s begin with the Mayo Clinic risk stratification model (where the risk refers to the risk of progression, not of having smoldering multiple myeloma (SMM) or multiple myeloma (MM) at time of bone marrow exam). It defines risk groups on the basis of three abnormal parameters:
- Parameters include:
- IgG MGUS
- M protein concentration below 15 g/L (1.5 g/dL)
- FLC ratio between 0.26 and 1.65
- Number of parameters (risk for progression at 20 years):
- 0 low-risk (5%)
- 1 low-intermediate risk (21%)
- 2 high-intermediate risk (37%)
- 3 high risk (58%)
This patient, then, has a low-intermediate risk. The following table reviews recommendations as to whether or not to perform a bone marrow aspirate and biopsy, based on expert opinion and clinical practice guidelines:
| Source | Indication for bone marrow |
|---|---|
| Gonsalves and Rajkumar, 2022 | Recommended (because of the IgA) |
| Go and Rajkumar, 2017 | Recommended (because of the IgA) |
| Mickael, 2014 | May be deferred because M protein concentration is low (less than 0.5 gm/dL) |
| UptoDate | Recommended (because of the IgA) |
| UKMF/NMSG/BSH | At the discretion of the myeloma team |
| EMN | May be considered |
| IMWG | Recommended (because of the IgA) |
| iStopMM risk model | May not be necessary (see calculation below) |
Let’s now consider the iStoMM risk model, which is described in more detail in a study summary below. To use this model in our patient, we need the following information:
- MGUS isotype – IgA
- M protein concentration – 0.45 g/L
- Free light chain ratio – 1.0
- Total IgG – not stated in the case, let’s assume 10 g/L
- Total IgA – not stated in the case, let’s assume 4.5 g/L
- Total IgM – not stated in the case, let’s assume 1 g/L
Let’s plug these numbers into the iStopMM calculator:
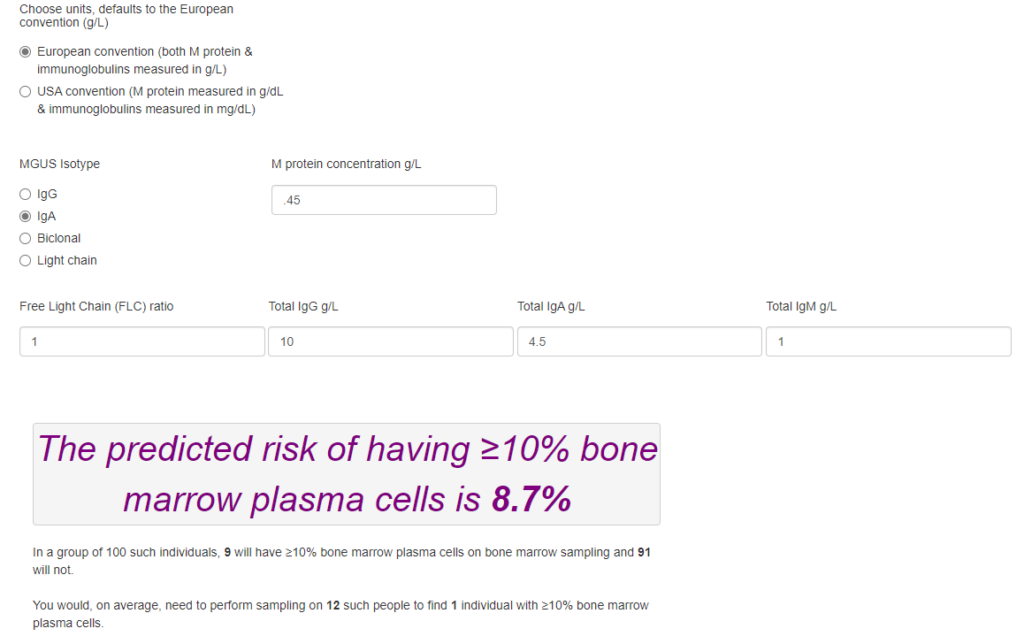
The authors of the study that describes this new mode chose <10% as a low-risk threshold (for predicting (risk of > 10% bone marrow plasma cells) in which bone marrow sampling could safely be deferred,1 so this patient would be spared a bone marrow examination. In contrast, he qualifies as low-intermediate risk based on the Mayo Clinic model (because of the IgA isotype) and so would generally be recommended to have a bone marrow examination. This discrepancy is consistent with the authors’ conclusion that: “For any plausible low-risk threshold, our prediction model identifies a higher proportion of persons with MGUS as being low-risk for SMM or worse with a higher negative predictive value than does the Mayo Clinic risk stratification model.”
Introduction
- By definition MGUS requires bone marrow clonal plasma cells <10% and no evidence of lytic lesions on skeletal imaging, not all patients with suspected MGUS need these tests performed.
- Arguments for performing a bone marrow biopsy on patients with MGUS:
- It is required to distinguish between persons with presumed MGUS and those with SMM/MM, both of which are potentially treatable.
- It provides prognostic information.
- Arguments against performing a bone marrow biopsy on patients with MGUS:
- Only a small percentage of patients with MGUS will prove to have SMM, and an even much smaller (negligible) number will have MM.
- Bone marrow sampling can be painful and is associated with rare complications.
- It is generally performed only at specialized centers.
- The extent to which a bone marrow examination contributes to a change in management has not been well established.2
- Efforts should be made to identify persons who are unlikely to benefit from the procedure to minimize harm and costs. A decision to perform a bone marrow examination may be supported by the creation of risk groups, of which the Mayo Clinic risk stratification model is the most commonly used. A more recent example is the iStoMM risk model, though it has not yet been validated or incorporated in clinical practice guidelines.
- Current clinical practice guidelines suggest that most persons with MGUS should undergo bone marrow sampling but that the procedure may be deferred in those classified as low-risk MGUS according to the Mayo Clinic model.3
Definitions
- MGUS is defined by:
- Smoldering myeloma (intermediate asymptomatic stage between MGUS and MM) is defined by:6
- M-spike (IgG or IgA ≥30 g/L, or urinary M-protein ≥500 mg per 24 h) and/or
- Clonal BMPC 10% to 59%, in the absence of myeloma-defining events or amyloidosis
- Diagnosis of multiple myeloma requires:7
- ≥10% clonal bone marrow plasma cells (BMPC) or a biopsy-proven plasmacytoma.
- Evidence of organ damage related to the disease, either of:
- CRAB criteria (one or more):
- Serum calcium increased > 1 mg/dL (0.25 mmol/L) above the upper limit of normal or > 11 mg/dL (2.75 mmol/L).
- Renal insufficiency with creatinine clearance < 40 mL/minute or serum creatinine level > 2 mg/dL (177 mcmol/L).
- Anemia with hemoglobin > 20 g/L [2 g/dL] below the lower limit of normal or hemoglobin < 100 g/L (10 g/dL).
- Bone lesions with ≥ 1 osteolytic lesions on skeletal radiography, computed tomography (CT), or positron emission tomography (PET)-CT.
- Validated biomarkers of malignancy (one or more):
- Clonal plasma cell percentage on bone marrow exam, preferably from a core biopsy specimen, of ≥ 60%.
- Serum involved to uninvolved free light chain (FLC) ratio of ≥ 100 if the absolute level of involved light chains is ≥ 100 mg/L using flow cytometry, immunohistochemistry, or immunofluorescence.
- More than 1 focal lesion on magnetic resonance imaging (MRI) that are ≥ 5 mm in size.
- CRAB criteria (one or more):
Risk stratification
- Mayo Clinic risk stratification model:
- Mayo Clinic risk stratification model for MGUS defines risk groups on the basis of the number of abnormal parameters:
- Parameters include:
- IgG MGUS
- M protein concentration below 15 g/L (1.5 g/dL)
- FLC ratio between 0.26 and 1.65
- Number of parameters (risk for progression at 20 years):
- 0 low-risk (5%)
- 1 low-intermediate risk (21%)
- 2 high-intermediate risk (37%)
- 3 high risk (58%)
- Parameters include:
- Mayo Clinic risk stratification model for SMM:
- Parameters include:
- M protein concentration > 2 g/dL
- FLC ratio between > 20
- BM plasma cells >20%
- Number of parameters:
- 0 low risk
- 1 intermediate risk
- 2-3 high risk
- Parameters include:
- Note from Eythorsson et al: “The [Mayo Clinic risk stratification] model was originally developed to stratify persons with MGUS into risk groups on the basis of their absolute risk for progression to MM or related disorders at 20 years. Since then, advances in imaging and changes in the definition of MM have likely rendered these risk estimates inaccurate. In current clinical practice, the model has been repurposed on the basis of expert opinion for use in the decision to obtain a bone marrow sampleith the recommendation that sampling may be deferred in persons classified as having low-risk MGUS. This was partially justified on the grounds that only 4.8% of those classified as low-risk MGUS in the derivation cohort turned out to have 10% or greater BMPC.”
- Mayo Clinic risk stratification model for MGUS defines risk groups on the basis of the number of abnormal parameters:
- See Eythorsson et al study summary below for a new iStopMM multivariable model to predict the need for bone marrow sampling.
Estimation of bone marrow plasma cells
- Based either on bone marrow aspirate or bone marrow trephine biopsy.
- IMWG recommends both bone marrow aspirate and bone marrow biopsy for plasma cell quantification, and if there is a discrepancy between BMPC% in the two methods, the higher of the two values should be used.8
Clinical studies
- Sidiqi et al, 2020
- Retrospective review of multiple myeloma (MM), smoldering multiple myeloma (SMM), and monoclonal gammopathy of undetermined significance (MGUS).
- Aim was to determine whether a bone marrow biopsy (BM) is necessary in all patients diagnosed with a monoclonal protein
- A total of 2254 MM, 397 SMM, and 5836 MGUS patients were included in the study according to the updated IMWG criteria
- Omitting a BM in a patient without laboratory abnormalities in hemoglobin, calcium, and renal function and who has low-risk MGUS will result in missed diagnosis of MM or SMM in <1% of patients.
- Eythorsson et al, 2024
- Objective: To develop a multivariable prediction model using commonly available laboratory parameters that predicts the probability that a person with presumed MGUS has 10% or greater BMPC and therefore a diagnosis of SMM or MM by bone marrow criteria to inform the decision to obtain a bone marrow sample and compare its performance to the Mayo Clinic risk stratification model
- Design:
- iStopMM (Iceland Screens, Treats or Prevents Multiple Myeloma), a prospective population-based screening study of MGUS.
- Proportional odds logistic prediction model was used.
- Mayo Clinic risk stratification model was used for comparison to the prediction model
- Setting: Icelandic population of adults aged 40 years or older.
- Patients: 1043 persons with IgG, IgA, light-chain, and biclonal MGUS detected by screening and an interpretable bone marrow sample.
- Measurements:
- Predictors included:
- Nonlinear variables:
- Monoclonal gammopathy of undetermined significance isotype
- Free light-chain ratio
- Linear variables:
- Monoclonal protein concentration
- Total IgG, IgA, and IgM concentration
- Nonlinear variables:
- Predictors included:
- Results:
- 15.1% persons had 10% or greater BMPC on sampling, of whom 98.7% had SMM and 1.3% had MM.
- Performance of the Prediction Model:
- The median predicted risk for SMM or worse by bone marrow criteria in the cohort was 7.7%
- Compared with IgG MGUS, the risk for SMM or worse was only slightly higher for:
- Biclonal MGUS (odds ratio [OR], 1.64 [95% CI, 1.11 to 2.44])
- IgA MGUS (OR, 1.48 [CI, 0.98 to 2.23])
- Light-chain MGUS (OR, 1.04 [CI, 0.60 to 1.80])
- By far the 2 strongest predictors of SMM or worse were:
- M protein concentration (OR between 3.9 g/L [75th percentile] and 2.1 g/L [median], 2.07 [CI, 1.63 to 2.63 g/L])
- FLC ratio (OR between 1.9 [75th percentile] and 1.2 [median], 1.29 [CI, 1.13 to 1.47])
- Use of the prediction model to defer bone marrow sampling if the predicted risk for SMM was below a 10% risk threshold would have resulted in sampling being deferred in 613 (58.8%) participants, of whom 22 (3.6%) would have SMM and none would have MM, yielding a negative predictive value of 96%.
- Of the remaining 430 (41%) who would have undergone sampling, 134 (31%) would have been found have SMM and 2 (0.47%) would have been found to have MM
- Mayo Clinic Risk Stratification Model:
- Proportion of SMM or MM by bone marrow criteria:
- Low-risk MGUS – 6.2% (CI, 4.2% to 9.1%)
- Low-intermediate risk MGUS – 16.1% ((CI, 12.9% to 19.9%
- High intermediate risk MGUS – 28.2% (CI, 22.8% to 34.3%)
- high risk MGUS – no patients
- Using the Mayo Clinic model to defer bone marrow sampling if the predicted risk for SMM or worse was below a threshold of 10% (equivalent to deferring sampling in those classified as low-risk MGUS), sampling would have been deferred in 386 (37%) participants, of whom 24 (6.2%) would have had SMM and none would have had MM. Of the 657 (63%) low-intermediate and high-intermediate risk participants who would have undergone sampling, 132 (20%) would have had SMM and 2 (0.3%) would have had MM.
- Proportion of SMM or MM by bone marrow criteria:
- The prediction model outperformed the Mayo Clinic model over a range of reasonable low-risk thresholds.
- Discussion:
- For any plausible low-risk threshold, our prediction model identifies a higher proportion of persons with MGUS as being low-risk for SMM or worse with a higher negative predictive value than does the Mayo Clinic risk stratification model, and consequently the net benefit of our model is always higher by a margin of 0.13 to 0.30.
- In this context, a net benefit of 0.30 is consistent with a strategy that reduces the number of unnecessary bone marrow sampling procedures by 300 for every 1000 persons with presumed MGUS, without missing a single additional case of SMM or worse.
- Persons with predicted risks below the relevant low-risk threshold could safely defer bone marrow sampling and be managed by primary care physicians as presumed MGUS.
- The model does not supersede clinical judgment and should only be used if there is no clinical suspicion of MM or related lymphoproliferative disorders, including light-chain amyloidosis.
- This accurate prediction model for SMM or worse was developed in a population-based cohort of persons with presumed MGUS and may be used to defer bone marrow sampling and referral to hematology.
- Clinical calculator at www.istopmm.com/riskmodel.
- Comment from UptoDate: In this population, the model had a 96 percent negative predictive value. If it were used to defer bone marrow sampling for those estimated to have <10 percent bone marrow involvement, it would allow 59 percent of the population to defer bone marrow, of whom 3.6 percent would have SMM and none would have MM upon biopsy The Mayo Clinic model recommends deferring a bone marrow evaluation in persons with low-risk MGUS and defines low-risk MGUS as IgG MGUS with monoclonal protein <1.5 gm/dL and normal FLC ratio. The iStopMM model uses entry of actual numeric values into the risk calculator. Positive and negative predictive values are directly related to the prevalence of disease in a population.

Expert opinion
- Gonsalves and Rajkumar, 2022:
- Bone marrow examination is not routinely recommended in patients with low-risk MGUS.
- A bone marrow examination is not required for patients who have MGUS with features suggesting low risk for progression.
- Go and Rajkumar, 2017:
- A bone marrow can be deferred in patients with:
- Small (<1.5 gm/dL) IgM MGUS
- Low-risk MGUS (IgG type, M protein <1.5 gm/dL, normal free light-chain ratio)
- Small (involved/uninvolved serum-free light-chain ratio <8) light-chain MGUS in whom there are no clinical features concerning for myeloma or lymphoplasmacytic malignancy.
- Routine bone marrow biopsy in low-risk MGUS has a low yield.
- Avoiding bone marrow biopsy in these patients will minimize health care costs without adversely affecting clinical outcome.
- Similarly, a baseline bone marrow biopsy can also be omitted in patients with apparently asymptomatic IgM MGUS who have a small quantity of M-protein (<1.5 gm/dL) and normal blood counts because the probability of finding an LPM needing therapy is very low.
- Although data on light-chain MGUS are lacking, we do not recommend routine skeletal imaging and bone marrow evaluation in patients who have a low involved/uninvolved FLC ratio (<8) in whom there are no clinical concerns for LPMs.
- For all other patients with MGUS bone marrow biopsy at the time of diagnosis.
- A bone marrow can be deferred in patients with:
- Mickael, 2014:
- Bone marrow aspirate and biopsy:
- Recommended in higher-risk cases:
- M-protein concentration >1.5 gm/dL
- IgM-MGUS)
- May be deferred in:
- Very elderly
- Those in whom the M protein concentration is low (less than 0.5 gm/dL)
- Patients with an inflammatory condition
- Recommended in higher-risk cases:
- Bone marrow aspirate and biopsy:
- UptoDate:
- Bone marrow evaluation can be deferred in individuals with no evidence of anemia, lymphadenopathy, or organomegaly with the following low-risk scenarios:
- IgG monoclonal protein <1.5 g/dL (15 g/L) with normal FLC ratio
- Light chain only monoclonal protein with FLC ratio <8
- IgM monoclonal protein <1.5 g/dL (15 g/L)
- <10 percent bone marrow involvement estimated by iStopMM risk model
- Bone marrow evaluation can be deferred in individuals with no evidence of anemia, lymphadenopathy, or organomegaly with the following low-risk scenarios:
Guideline Recommendations
- UK Myeloma Forum (UKMF) and Nordic Myeloma Study Group (NMSG)/on Behalf of British Society of Haematology:
- In patients with presence of a low-level M-protein (< 15 g/L) plus normal full blood count, renal and bone function, normal uninvolved immunoglobulins and the absence of symptoms, multiple myeloma or related disorder is unlikely to be present and bone marrow examination may or may not be carried out at the discretion of the myeloma team.
- Exceptions may include patients:
- With:
- Anemia
- Renal impairment
- Osteopenia
- Isolated vertebral collapse
- M protein level is ≥ 10-20 g/L
- M protein and suspected of having a:
- Malignant plasma cell disorder
- Other lympho-proliferative disorder
- AL amyloidosis
- < 60 years old
- With:
- European Myeloma Network (EMN):
- Routine bone marrow exam not recommended in asymptomatic patients with:
- All of:
- Apparent IgG MGUS
- Serum M protein ≤ 15 g/L
- No end organ damage
- Suspected light chain MGUS except those with high levels of involved light chain (for example, free light chain ratio > 10).
- All of:
- Consider bone marrow examination for all patients with IgA and IgM M proteins.
- Routine bone marrow exam not recommended in asymptomatic patients with:
- International Myeloma Working Group (IMWG) Consensus:
- Bone marrow examination not recommended for low-risk MGUS.9
- Perform bone marrow examination if:
- Monoclonal protein >15 g/L
- IgA or IgM protein type
- Abnormal FLC ratio
- Bone marrow examination is always required if a patient with presumed MGUS has unexplained anemia, renal insufficiency, hypercalcemia, or bone lesions or a suspicion of AL amyloidosis.
- International Expert Consensus:
- No consensus regarding requirement for BM aspirate and biopsy for patients diagnosed with monoclonal gammopathy:
- Half of the panel suggested bone marrow examination for MGUS patients with higher levels of M proteins (>15 g/L) and abnormal FLC ratios since they are more likely to have multiple myeloma or other serious B cell disorder
- Other panel members recommended that all patients with a monoclonal gammopathy, regardless of the size of the initial M-spike, should undergo bone marrow examination.
- No consensus regarding requirement for BM aspirate and biopsy for patients diagnosed with monoclonal gammopathy: