Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
A page from the hematology fellow late in the evening is rarely about the laboratory value.
It is about the distance between data and decision.
The platelet count is 24.
The patient is stable.
There is no active bleeding, no accelerating physiology.
And yet the page comes.
“What should we do?”
The question is about platelets.
Ultimately, it is about uncertainty.
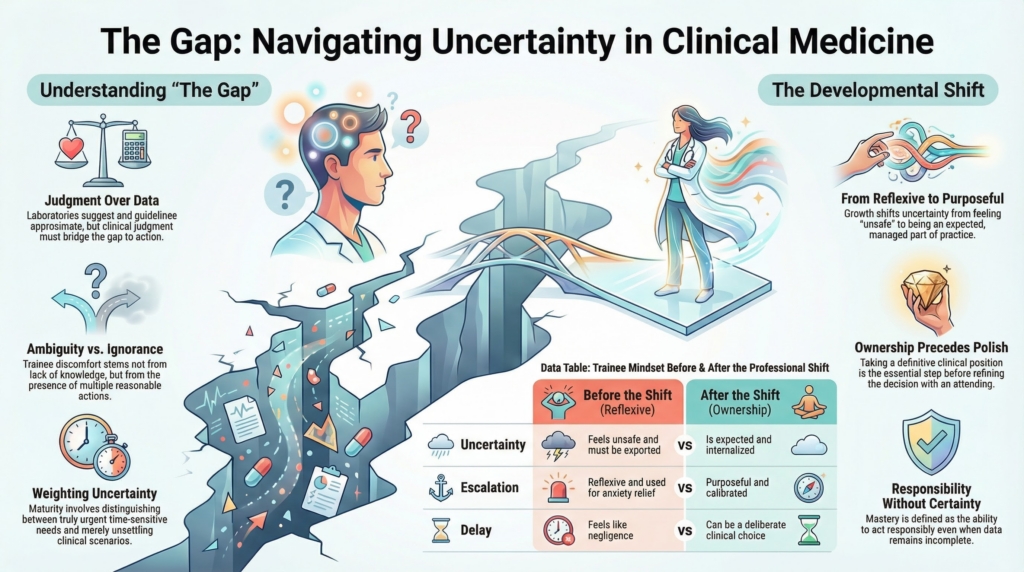
The Gap
Clinical medicine lives in a gap.
Data rarely dictate action.
Laboratories suggest.
Imaging implies.
Guidelines approximate.
Between information and intervention sits judgment.
For many trainees, that gap is destabilizing.
They are not confused about the facts.
They are uncomfortable occupying the space where more than one reasonable action exists.
The discomfort is not ignorance.
It is ambiguity.
The page, in effect, is a request to share that discomfort.
The Hidden Threshold
At some point in training, a quiet shift must occur.
Before the shift:
- uncertainty feels unsafe
- escalation feels protective
- silence feels negligent
After the shift:
- uncertainty is expected
- delay can be deliberate
- escalation is purposeful rather than reflexive
The difference is not knowledge.
It is ownership.
The fellow who asks, “What should we do?” is still transferring the burden of decision, as early trainees understandably do.
The fellow who says, “I think we should observe overnight. She is stable, there are no high-risk features, and we can reassess in the morning,” has crossed a developmental line.
The attending may agree or refine.
But a position has been taken.
Ownership precedes polish.
That line is rarely crossed once. It is crossed, retreated from, and crossed again until it holds.
Why This Is Hard
Many trainees have been rewarded their entire lives for correctness.
Exams had answers.
Performance had metrics.
Mastery meant precision.
Speed and certainty were treated as signs of competence.
Consult medicine changes the terms.
Now the task is not to be right with certainty.
It is to act responsibly without it.
That requires tolerating three realities:
- the data will be incomplete.
- reasonable clinicians will disagree.
- responsibility cannot be deferred indefinitely.
When ambiguity produces immediate escalation, relief follows. Anxiety decreases.
But judgment does not mature.
Confidence in medicine is retrospective.
It forms after decisions are made and outcomes observed.
The page is answered.
The skill is not built.
Urgent Versus Uncomfortable
A central error in early clinical development is conflating urgency with discomfort.
Some decisions are time-sensitive.
Many are merely unsettling.
Distinguishing the two is foundational.
If every uncomfortable decision is treated as urgent, the system saturates with unnecessary escalation.
If true urgency is minimized, harm follows.
The first exhausts the system.
The second endangers patients.
The work is not eliminating uncertainty.
It is weighting it.
Uncertainty Does Not Disappear
It is tempting to imagine that tolerance of ambiguity arrives with seniority. It does not. It changes terrain.
Even experienced clinicians feel anxiety when the clinical ground shifts beneath them. A benign hematologist confronted with acute leukemia may feel the tightening that accompanies high-stakes disease. The presence of anxiety is not the issue.
The difference is structural.
Knowing when to call malignant hematology colleagues is not avoidance. It is calibrated response. The uncertainty is acknowledged, bounded, and scaffolded.
Professional steadiness is not emotional numbness. It is clarity about the limits of one’s domain and confidence in the systems that support those limits.
The trainee experiences uncertainty about the patient.
The attending experiences uncertainty about timing, intervention, and scope.
Formation is learning to internalize uncertainty rather than export it reflexively.
Formation
The goal of training is not certainty.
It is steadiness inside uncertainty.
The fellow who becomes a colleague is not the one who knows the most.
It is the one who can stand in the gap between data and decision long enough to take responsibility for choosing.
The page becomes less frequent not because doubt disappears, but because doubt has been absorbed, examined, and acted upon.