In hereditary hemochromatosis (HH), excess iron accumulation is driven by increased absorption, not increased intake. Phlebotomy is the cornerstone of treatment. But should patients restrict dietary iron?
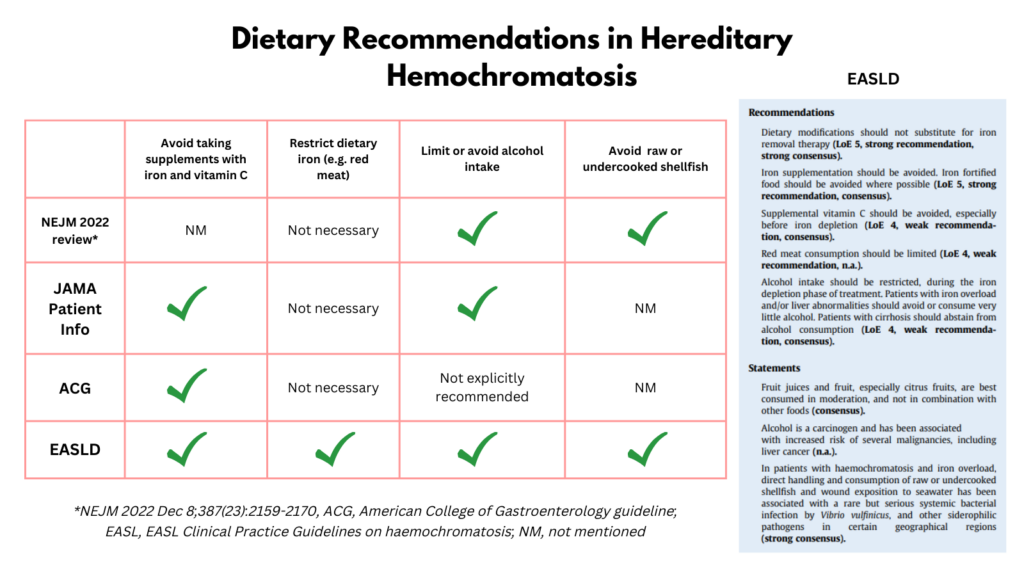
Guidelines differ. Some state that dietary restriction is unnecessary. Others suggest limiting red meat. The disagreement reflects something important: the effect size is modest.
This discussion applies to maintenance-phase HH, not the initial de-ironing phase, where weekly phlebotomy dwarfs any dietary contribution.
The math is smaller than most people think
In a typical maintenance-phase patient with HH:
- An unrestricted mixed diet might translate into roughly 6 maintenance phlebotomies per year.
- A meat-restricted diet might reduce that to about 4 per year.
- A vegetarian pattern might reduce it further.
The difference between unrestricted and meat-restricted intake is often on the order of 2–3 phlebotomies per year.
Diet does not eliminate the need for phlebotomy. It shifts frequency modestly.
To understand why recommendations diverge, it helps to quantify the effect of diet on iron balance.
Iron Balance Model in Hereditary Hemochromatosis
| Diet Type | Iron Intake (mg/day) | Absorption (%) | Iron Absorbed (mg/day) | Net Retained (mg/day)* | Iron Retained (mg/year) | Phlebotomies per Year** |
|---|---|---|---|---|---|---|
| Unrestricted mixed | 18 | 30% | 5.4 | 4.4 | 1606 | 6.4 |
| Meat-restricted | 12 | 30% | 3.6 | 2.6 | 949 | 3.8 |
| Vegetarian | 12 | 15% | 1.8 | 0.8 | 292 | 1.2 |
* Net retained = absorbed iron − 1 mg/day physiologic losses
** Assuming 250 mg iron removed per phlebotomy
Note: These estimates use simplified, rounded assumptions. Intake values reflect common Western ranges. Absorption fractions (≈30% heme-rich, ≈15% vegetarian) reflect known differences in bioavailability and enhancement by meat and vitamin C. These represent steady-state maintenance conditions; real-world absorption varies with genotype, iron stores, hepcidin levels, and inflammation.
The equation has changed
Historically, therapeutic phlebotomy units were discarded. Extra phlebotomies meant extra inconvenience with no broader benefit.
Today, many blood centers accept donations from patients with HH. Policies vary by region and center, and donation eligibility depends on meeting standard donor criteria. In that setting, “extra phlebotomies” may simply become “extra donations.”
That reframes the issue:
- Is the goal to minimize procedures?
- Or is periodic blood donation acceptable, even meaningful?
Clinical Tradeoffs in Maintenance HH
| Strategy | Procedural Burden | Dietary Burden | Societal Benefit | Primary Value Prioritized |
|---|---|---|---|---|
| Unrestricted diet + therapeutic phlebotomy | moderate | none | none | Convenience |
| Meat-restricted diet + therapeutic phlebotomy | lower | moderate | none | Fewer procedures |
| Unrestricted diet + blood donation | moderate | none | high | Societal contribution |
| Meat-restricted diet + blood donation | lower | moderate | moderate | Balance |
What does “iron restriction” actually mean?
It rarely means eliminating all iron-containing foods.
More commonly, it means:
- reducing red meat intake (heme iron)
- avoiding iron supplements and fortified foods
- moderating alcohol1
- avoiding vitamin C loading with high-iron meals
The most powerful lever is heme iron from red meat, not total iron grams on a nutrition label.
So what should we recommend?
For many patients in maintenance phase:
Dietary iron restriction is optional, not mandatory.
It becomes a preference-sensitive decision based on:
- access to blood donation
- tolerance of phlebotomy
- dietary preferences
- quality of life
Iron metabolism sets the physiology.
Patient values determine the plan.