Iron Deficiency Is Not Just Anemia
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Iron deficiency and anemia are often treated as interchangeable.
They are not.
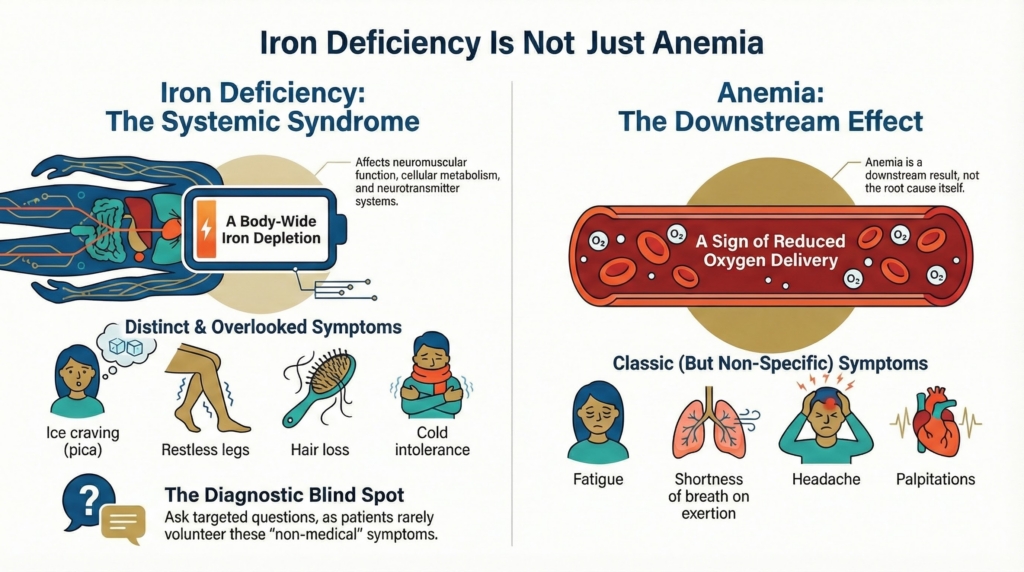
Anemia is a downstream manifestation.
Iron deficiency is an upstream systemic deficiency that can exist with or without anemia.
Anemia reflects reduced oxygen-carrying capacity.
Iron deficiency reflects depleted iron biology across multiple systems.
A patient can be profoundly iron deficient and not anemic.
And a patient can be anemic for reasons unrelated to iron deficiency.
Conflating the two narrows what clinicians listen for, what patients are asked, and which symptoms are taken seriously.
It also shapes which patients are told that nothing is wrong.
Iron deficiency is not just a laboratory abnormality.
It is a physiological syndrome.
And its most important manifestations often live in the history, not the hemoglobin.
Two overlapping syndromes with different symptom worlds
Iron deficiency and anemia share some symptoms.
But they also have distinct symptom profiles.
The classic symptoms of anemia, driven primarily by reduced oxygen delivery, tend to be:
- fatigue
- shortness of breath on exertion
- headache
- palpitations
- chest discomfort in patients with coronary disease
These are the classic anemia symptoms.
They are common.
They are nonspecific.
They reflect impaired oxygen delivery rather than iron-specific physiology.
Iron deficiency, by contrast, produces a different and richer symptom constellation.
Not because the symptoms are exotic.
But because they are physiologically coherent.
Common symptoms of iron deficiency include:
- pica (especially ice craving)
- restless legs
- hair loss
- brittle or abnormal nails
- glossitis or tongue discomfort
- cold intolerance
- tinnitus
- cognitive fog or difficulty concentrating
These symptoms can be severe even when hemoglobin is normal.
They reflect iron’s role in neuromuscular function, epithelial turnover, neurotransmitter systems, and cellular metabolism.
They are not psychological.
They are biological.
Why patients rarely volunteer these symptoms
One of the most striking features of iron deficiency is not just what patients feel.
It is what they don’t say.
Patients rarely volunteer classic iron-deficiency symptoms without being asked directly.
Not because they are hiding information.
But because many of these experiences do not naturally present themselves as “medical.”
Cold intolerance is often interpreted as personality or constitution.
“This is just how I am.”
Restless legs are difficult to describe.
Patients struggle to put words to an urge rather than a pain.
Hair loss is normalized or attributed to stress, aging, or hormones.
Pica carries shame, secrecy, and sometimes pleasure.
Patients often don’t volunteer it at all.
When asked directly, the reaction is often unmistakable.
Wide-eyed recognition.
A half-smile.
A sense of being seen.
“How did you know?”
That moment is not magic.
It is expert history-taking.
Expert history is not about asking more questions — it is about asking different questions
Expert history-taking in iron deficiency is not about open-ended wandering.
It is about physiologically informed, targeted questioning.
Not because the symptoms are rare — and because patients rarely volunteer them.
But because they are specific.
Direct questions about:
- ice craving
- restless legs
- hair or nail changes
- tongue discomfort
- cold sensitivity
- tinnitus
are not fishing expeditions.
They are hypothesis-driven probes.
They turn vague discomfort into recognizable physiology.
They uncover a syndrome that patients often carry silently.
This is not about being thorough.
It is about being precise.
When hemoglobin defines permission — and the misogyny of iron deficiency
One of the most common stories in iron deficiency is this:
One of the most common stories in iron deficiency is this:
A young menstruating patient reports ice craving, restless legs, hair loss, cold intolerance, and fatigue.
A CBC is checked.
The hemoglobin is normal.
The patient is told, “Your blood is fine.”
This is not because the clinician is careless.
It is because hemoglobin has been culturally trained to function as permission.
Permission to investigate.
Permission to validate symptoms.
Permission to label a problem as real.
When hemoglobin is normal, iron deficiency is often not considered.
And when iron deficiency is not considered, the patient’s physiology is quietly reinterpreted as personality, stress, anxiety, or normal variation.
What feels to patients like dismissal is often, from the clinician’s side, a conceptual artifact.
It reflects how iron deficiency has been taught, operationalized, and subordinated to hemoglobin.
This pattern has been described as the misogyny of iron deficiency.
Not because individual clinicians are misogynistic.
But because the system has been trained to listen to hemoglobin and not to iron biology.
Young women reporting ice craving, hair loss, restless legs, and cold intolerance are often told that nothing is wrong when their hemoglobin is normal.
Their symptoms are minimized.
Their physiology is psychologized.
Their experience is reframed as stress, anxiety, or normal variation.
The result is a predictable sequence:
- real physiological symptoms
- normal hemoglobin
- dismissal or normalization
- delayed diagnosis
- delayed treatment
This is not a moral failure.
It is a conceptual one.
Iron deficiency has been framed as a subset of anemia.
When in fact, anemia is a subset of iron deficiency’s possible consequences.
Non-anemic iron deficiency is a physiological syndrome.
It can be highly symptomatic.
But because it does not meet the traditional threshold of anemia, it often falls into a diagnostic blind spot.
For patients, this can feel like disbelief or invalidation.
For clinicians, it is usually an artifact of training, guidelines, and laboratory-centered definitions of disease.
What feels personal is often structural.
Pica is not a quirky symptom — it is diagnostic intelligence
Symptom awareness carries both burden and benefit.
On the one hand, symptoms like pica can be distressing, socially stigmatizing, and physically disruptive.
On the other hand, they provide early warning.
Pica is not just a craving.
It is diagnostic intelligence.
For many patients, the return of ice craving is the earliest marker of recurrent iron deficiency.
Often earlier than laboratory confirmation.
Patients learn their own physiology before the system does.
They call not because a lab was abnormal.
They call because they are eating ice again.
In this sense, pica functions as a biomarker.
A lived biomarker.
One that does not appear on a flowsheet.
But one that is often more sensitive than a scheduled ferritin.
There is also something quietly powerful about this.
Pica gives patients agency.
They are not waiting for the system to tell them something is wrong.
They recognize recurrence in real time.
They are reminded that they know their own bodies.
They are no longer passive recipients of laboratory interpretation.
They become active participants in monitoring their own condition.
This knowledge allows:
- earlier testing
- earlier treatment
- earlier relief
This is a form of embodied monitoring.
It is not captured in guidelines.
But it is real.
This is not quirky behavior.
It is diagnostic intelligence.
Lived, embodied, and often earlier than the system is prepared to see.
Urgency without hemoglobin
Urgency in iron deficiency is not always about hemoglobin.
I once cared for a patient with severe pica who had been eating toilet paper compulsively.
She presented with esophageal obstruction and hypersalivation and required urgent endoscopic removal.
She also received urgent intravenous iron.
Within days, her cravings resolved.
Not because her hemoglobin demanded it.
But because her physiology did.
In another case, a patient consuming five to five pounds of ice per day developed severe hyponatremia in the setting of SIADH.
She was hospitalized for electrolyte derangement driven not by anemia, but by iron-deficiency-driven behavior.
Again, intravenous iron was urgent.
Not because of oxygen delivery.
But because of systemic risk created by iron-deficient physiology.
Iron deficiency can create clinical urgency even when traditional anemia thresholds would not.
Urgency is not always a hemoglobin problem.
Sometimes it is a systems problem.
Why iron deficiency histories are so interesting
One of the joys of caring for patients with iron deficiency is that their histories are often rich, specific, and physiologically revealing.
They are not vague.
They are patterned.
They tell a story of cellular iron biology playing out across multiple systems.
They are often more interesting than the anemia itself.
Fatigue and dyspnea are generic.
Pica, restless legs, glossitis, cold sensitivity, tinnitus, hair and nail changes are not.
They are signatures.
They are the body speaking a specific language.
Expert clinicians learn to hear it.
Iron deficiency as a physiological syndrome
Iron deficiency is not just a low ferritin.
It is a systemic state.
It affects:
- epithelial turnover
- neuromuscular signaling
- dopaminergic pathways
- thermoregulation
- cellular metabolism
- mucosal integrity
That is why its symptoms are diverse.
That is why its manifestations are often more striking than the anemia it may or may not cause.
That is also why treating iron deficiency can produce dramatic symptomatic improvement even when hemoglobin changes little.
Patients often feel better before their CBC looks better.
That is not placebo.
That is physiology.
What expert history-taking makes visible
Expert history-taking in iron deficiency does not just uncover symptoms.
It restores coherence.
It tells patients:
What you are experiencing makes sense.
There is a biological explanation.
You are not imagining this.
For many patients, that validation is as powerful as the iron itself.
Because for months or years, their physiology has been speaking.
And no one has been listening in the right language.