The cognitive environments that determine what we see, weigh, and miss
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
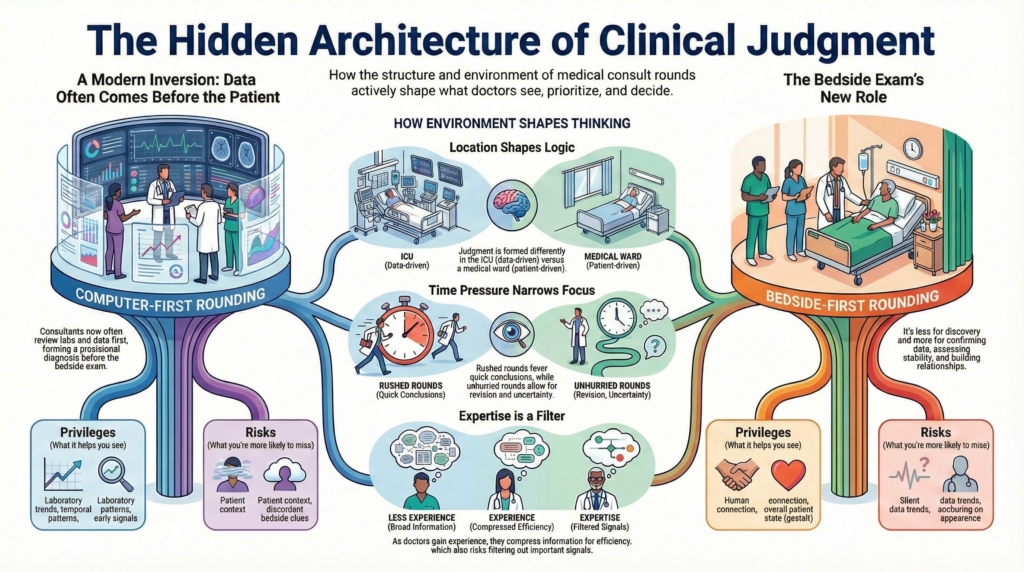
Every rounding structure creates a cognitive environment.
It privileges certain kinds of information and backgrounds others. It determines what is seen first, what is weighted heavily, what is deferred, and what may never quite enter the frame. Over time, these structures shape not only workflow, but judgment itself.
In modern inpatient hematology, consult rounds are no longer simply a way to visit patients. They are a way of organizing reality.
The inversion of discovery
Historically, the bedside encounter came first. The patient was examined. Findings were gathered. Data followed.
In contemporary consult practice, that sequence is often inverted.
Before entering the room, the consultant usually already knows:
- the CBC and trends
- the smear description
- the ferritin, LDH, creatinine, INR
- the trajectory over hours to days
- the unit location and clinical stability
By the time the consultant sees the patient, a provisional terrain has already been defined.
This changes the function of the bedside exam.
The exam is no longer primarily for discovery. It is often for:
- confirmation or contradiction of what the data suggest
- assessment of toxicity and physiologic stability
- detecting rare discordant findings that reframe terrain
- relationship-building and legitimacy in the patient’s eyes
In Consult Practice terms, Orientation is often data-informed before it is bedside-informed.
We no longer enter the room to discover what kind of problem this is.
We enter the room to test, humanize, and sometimes challenge the terrain we already think we’re in.
This is not laziness. It is a structural shift in how medicine functions when high-resolution, real-time data precede the bedside.
Bedside-first vs computer-first rounds
Some teams structure rounds around the patient. Others structure rounds around the chart.
Each structure privileges different cognitive work.
Bedside-first rounds tend to privilege:
- gestalt assessment of illness
- human connection and trust
- shared reality among the team
- subtle clinical instability
They risk:
- underweighting silent trends
- anchoring on appearance
- delayed integration of trajectory
Computer-first rounds tend to privilege:
- laboratory trends
- temporal patterns
- physiologic trajectories
- early signal detection
They risk:
- distancing from patient context
- overconfidence in numbers
- under-recognition of discordant bedside clues
Neither is inherently superior.
Each creates a different terrain of attention.
The danger is not choosing one style.
The danger is failing to recognize what each style makes more likely to be seen and more likely to be missed.
When presentation replaces presence
I once encountered a striking illustration of how rounding structure can quietly replace reality.
A resident confidently presented a consult patient as female. The story was polished. The clinical reasoning was fluent. The case seemed settled.
When we walked into the room, the patient was male.
It became immediately clear that the presenter had not actually seen the patient.
This was not dishonesty. It was structural drift.
The presentation had become a surrogate for presence. The chart had become a proxy for reality. The cognitive environment had allowed a polished narrative to substitute for physical encounter.
It was a reminder that in some rounding structures, seeing the patient becomes optional — and that this optionality carries real cognitive risk.
Presentation compression as cognitive terrain
How a case is presented is not neutral.
It determines what enters the shared cognitive field and what is silently assumed away.
Medical students are trained to present the full history and physical.
This is not inefficiency.
It is epistemology.
They are learning what might matter.
Residents begin to compress.
They learn to summarize, prioritize, and filter.
They begin to decide what is probably irrelevant.
Fellows compress further.
A fellow may present a short, elegant case.
Key labs.
Key symptoms.
A focused assessment.
The rest is assumed to have been checked.
Social history.
Medication lists.
Negative reviews of systems.
Their absence is taken to mean absence of relevance.
This is usually appropriate.
It is also a cognitive risk.
Compression trades breadth for efficiency.
It speeds Orientation.
It sharpens focus.
But it also narrows the field of possible signal.
Over time, teams learn not only how to present.
They learn what kinds of information are allowed to matter.
What gets compressed is not just detail.
It is possibility.
This is not a criticism of fellows.
It is a description of how expertise reshapes cognitive terrain.
Expertise teaches you what to ignore.
It also quietly teaches you what you may never see.
Unit geography as cognitive terrain
Consult rounds are not uniform across the hospital.
Different units impose different cognitive and practical constraints.
In the ICU:
- patients are often intubated
- lines, monitors, and sedation dominate the visual field
- waking the patient for exam may be inappropriate
- physiologic reserve is often already threatened
Here, data and trajectory legitimately dominate Orientation. The bedside exam is often secondary, focused on stability rather than discovery.
On the medical ward:
- patients are accessible
- subtle changes in appearance may matter
- history and exam may meaningfully shift terrain
In the emergency department:
- tempo dominates
- uncertainty tolerance is low
- early Orientation is provisional and rapidly revised
On labor and delivery:
- access is restricted
- locked doors and security procedures delay bedside presence
- patient flow and urgency reshape what is feasible
- consult entry itself becomes a friction point
These environments do not just change logistics.
They change how judgment is formed.
Time as cognitive terrain
Not only where rounds occur, but when they occur shapes cognition.
Early morning rounds, compressed by operating room schedules and clinic start times, tend to privilege efficiency, heuristics, and rapid synthesis.
Later rounds, when time pressure is lower, more easily permit deliberation, second looks, and explicit reassessment of trajectory.
Rushed rounds favor closure.
Unhurried rounds permit revision.
Time pressure is not just a logistical constraint.
It is a cognitive force that shapes how much uncertainty can be tolerated and how readily assumptions are revisited.
Patient and family presence
When patients and families are present during rounds, the cognitive environment changes again.
What can be said out loud shifts.
How uncertainty is expressed shifts.
Whether trainees speak freely shifts.
In these settings, consultants may perform confidence, suppress provisional thinking, or delay explicit discussion of uncertainty.
This does not make bedside rounds worse.
It makes them different.
Family presence alters not just communication.
It alters what kinds of reasoning are socially safe to display.
That, too, becomes part of the rounding terrain.
Language and interpreters as cognitive terrain
Language is not a neutral conduit for clinical information.
When care is mediated through an interpreter, the cognitive environment of the consult changes.
Not only what is said.
But how it is said.
How long it takes.
How much nuance survives.
Interpreted encounters reshape:
- the tempo of the visit
- the granularity of symptom description
- the patient’s ability to narrate chronology and sensation
- the clinician’s ability to probe and clarify
- the shared sense of uncertainty
History becomes slower.
Clarification becomes more effortful.
Subtle symptom qualities are harder to explore.
The consultant may default more quickly to data.
The bedside story may carry less weight.
Laboratory and imaging findings may silently rise in cognitive authority.
This is not because interpreters are ineffective.
It is because interpretation changes the structure of interaction.
Even with excellent interpreters, certain kinds of clinical information are more fragile:
- sensory descriptors
- embodied experiences
- temporal nuance
- emotional shading
- ambiguous or culturally specific symptoms
In these encounters, consultants may unconsciously simplify questions, truncate exploration, or accept vaguer answers than they would in a shared-language visit.
This can subtly narrow Orientation.
It can also increase reliance on “objective” data, not because the data are more accurate, but because they are more accessible.
Interpreter use does not make clinical judgment worse.
But it makes it different.
Recognizing this allows consultants to adjust:
- slowing down intentionally
- probing with more specificity
- checking understanding more explicitly
- protecting space for narrative even when it costs time
Language access is not just an equity issue.
It is a cognitive architecture issue.
It shapes what can be known.
Physical barriers and protective equipment
Precautions, isolation, gowns, masks, and eye protection are not cognitively neutral.
They:
- slow entry into rooms
- limit team size at the bedside
- fragment shared observation
- subtly discourage repeated bedside reassessment
In these settings, fewer people may enter. More discussion may occur outside the room. The bedside becomes less central to shared Orientation.
These are not just infection-control decisions.
They are structural modifiers of collective clinical perception.
The microscope as a rounding space
For hematology, the microscope is its own cognitive environment.
Who drives the microscope matters.
When the fellow drives:
- the fellow frames the field
- the fellow controls what is seen
- the fellow’s Orientation becomes upstream of the attending’s
When the attending drives:
- the attending curates attention
- subtle teaching points may surface
- hierarchy shapes what is emphasized
Where the microscope sits in rounds also matters:
- early, as an Orientation anchor
- late, as confirmation
- or separately, as a parallel cognitive stream
The microscope is not just a tool.
It is a site where Orientation and Thinking are socially constructed.
Technology and the redistribution of urgency
The iPhone has quietly reshaped consult practice.
Fellows can now photograph peripheral smears and transmit them instantly. What once required the attending to come in overnight now often becomes a text message exchange.
This has clear benefits. It reduces unnecessary overnight presence. It improves efficiency. It democratizes access to morphology.
But it also subtly shifts the meaning of urgency and presence.
The attending may see the smear without seeing the patient.
Diagnostic presence becomes portable.
Relational and contextual presence may recede.
Technology compresses some forms of urgency while diluting others.
Clinical responsibility is not removed.
It is redistributed — across distance, across devices, and across different forms of presence.
Team size and cognitive multiplication
The size and composition of the consult team matters.
A single fellow alone carries the full cognitive and logistical load. Teaching diminishes. Shared interpretation narrows. Fatigue compounds.
Larger teams change the cognitive environment:
- more eyes on the data
- more perspectives on morphology
- more opportunity for teaching and calibration
- more capacity to see patients promptly
The presence of visiting or international medical students adds another layer. It introduces different training cultures, different assumptions, and different ways of seeing clinical problems.
These are not just social benefits.
They are cognitive multipliers.
Pathology and blood bank as distributed rounding spaces
A collaborative clinical pathology department and blood bank are not peripheral to consult hematology. They are extensions of it.
These are not bedside rounds, but they function as distributed rounding spaces where Orientation and Execution are jointly constructed.
At institutions where hematologists can freely review slides at a multi-headed microscope with pathologists, shared interpretation becomes routine.
Similarly, an accessible blood bank transforms how consultants think about:
- transfusion reactions
- complex antibody patterns
- plasma exchange logistics
- sickle cell transfusion strategy
- urgent hemostatic support
These relationships change how quickly uncertainty is resolved and how safely Execution unfolds.
They are not ancillary services.
They are embedded cognitive partners.
Culture: deference versus challenge
Training culture shapes how consult judgment is received.
In systems influenced by oral examination traditions (for example, in Canada where I trained), consultants are often challenged. Recommendations are debated. Justifications are demanded. The interaction is adversarial in form but collaborative in spirit.
In many U.S. academic centers, the opposite is common. Consulting teams are deferential. Recommendations are accepted with little pushback.
This deference feels efficient. It also carries risk.
When consultants are never challenged, their errors go untested.
When teams never push back, collective reasoning weakens.
Deference can quietly replace shared responsibility.
A healthy consult culture does not require conflict.
It requires permission to think independently in the presence of authority.
Institutional boundaries and distorted terrains
Service boundaries also shape consult judgment.
At some institutions, benign and malignant hematology are structurally separated. Geography, coverage rules, and institutional politics determine who sees which patients.
This can create distorted terrains where consultants see patients outside their true expertise, manage temporary ownership of problems, and rely on remote colleagues for guidance.
These arrangements are rarely designed for cognition.
They are designed for coverage.
But coverage structures become cognitive structures. They determine who frames the problem, who sets posture, and who owns Execution in moments of uncertainty.
There is a parallel version of this problem at the boundary between hematology and vascular medicine.
In many institutions, vascular medicine primarily sees arterial disease, while hematology primarily sees venous disease.
But large-vein thrombosis and pulmonary embolism do not respect that distinction.
Iliac vein thrombosis.
Extensive femoral clot.
Submassive or massive pulmonary embolism.
These live in the borderlands.
Depending on institutional structure, any of the following may happen:
- vascular medicine is consulted first
- hematology is consulted first
- both services are consulted
- neither service clearly owns the problem
This is not because the physiology is ambiguous.
It is because the institutional map is.
When both services are involved, there is often:
- duplicated data review
- parallel risk stratification
- overlapping recommendations
- subtle differences in emphasis
- unclear ownership of final posture and execution
The patient may be discussed twice.
The team may hear two versions of the same story.
Responsibility becomes shared in theory and diffuse in practice.
This is not inefficiency alone.
It is a cognitive artifact of service boundaries.
The clot has one physiology.
The institution has two maps.
Which map is applied shapes:
- how aggressively risk is framed
- whether bleeding or thrombosis is weighted more heavily
- who owns anticoagulation strategy
- how escalation is handled
- how complications are interpreted
These borderland cases reveal something important:
Consult judgment is not only shaped by disease.
It is shaped by which service’s conceptual framework gets to define the terrain.
When physiology falls between services, cognition often fragments.
Redundancy is not accidental.
It is structural.
And in those spaces, clarity of ownership, posture, and execution becomes harder — not because the case is harder, but because the map is.
When a team insists on a consult you believe is inappropriate
Not every consult request reflects clinical necessity.
Some reflect anxiety.
Some reflect uncertainty.
Some reflect institutional habit.
Some reflect defensive medicine.
Some reflect misaligned ownership.
Being consulted does not obligate intellectual ownership.
One of the quiet skills of consult practice is recognizing when a problem is being handed off not because it is hematologic, but because it is uncomfortable.
This creates a distorted terrain:
The consultant is asked to solve a problem that is not truly within their domain.
The primary team offloads cognitive responsibility.
The consult becomes symbolic rather than substantive.
In these moments, the central judgment is not medical.
It is boundary judgment.
The consultant must decide:
Is this a hematology problem?
Or is this a medicine problem being externalized?
Saying “this is not a hematology problem” is not dismissiveness.
It is an act of cognitive clarity.
It protects:
- the integrity of consult reasoning
- the primary team’s ownership of their patient
- the consult service from becoming a catch-all for discomfort
This is not about refusing work.
It is about preserving accurate problem framing.
Consult services that never say no gradually become services that see everything — and therefore own nothing.
Over time, this dilutes both expertise and accountability.
Expert consultants learn that declining a consult can be as cognitively active as accepting one.
When authority pressure reshapes clinical posture (or similar)
Not all consult interactions are neutral.
Sometimes the referring attending is senior.
Sometimes they are forceful.
Sometimes they are certain.
Sometimes they are wrong.
Authority does not just transmit information.
It reshapes posture.
Junior consultants may feel pressure to:
- agree prematurely
- avoid reframing
- soften disagreement
- accept a terrain they do not believe is accurate
This is not weakness.
It is a predictable social force.
Hierarchy changes how much uncertainty is tolerated.
It changes how readily alternative frames are voiced.
It changes whether Thinking remains independent or becomes deferential.
The danger is not disagreement.
The danger is silent agreement.
When authority suppresses reframing, consult medicine quietly becomes execution of someone else’s thinking.
That is not consultation.
That is delegation.
Expert consult practice requires the capacity to say, respectfully and clearly:
“I see this differently.”
“I don’t think this is the right frame.”
“I’m concerned this assumption may be wrong.”
This is not confrontation.
It is intellectual stewardship.
Consultants are not there to rubber-stamp.
They are there to test, refine, and sometimes resist the prevailing frame.
Hierarchy should not be allowed to replace judgment.
Emotional intensity and the distortion of reasoning (for difficult patients)
Some consults arrive carrying more than physiology.
They carry:
- fear
- anger
- frustration
- mistrust
- prior bad experiences
- high emotional temperature
Difficult patients are not just difficult people.
They create difficult cognitive environments.
Emotion alters how information is processed.
It narrows attention.
It amplifies perceived urgency.
It increases pressure to act.
This can distort terrain in predictable ways:
- benign findings feel dangerous
- uncertainty feels intolerable
- closure is rushed
- thinking collapses into action
In these cases, the consultant is not only managing disease.
They are managing cognitive noise.
Recognizing emotional intensity as a terrain modifier is a core consult skill.
The question is not only:
What is happening physiologically?
It is also:
What emotional forces are shaping how this problem is being framed?
Sometimes the most important intervention is not diagnostic.
It is stabilizing the cognitive environment.
Slowing the tempo.
Naming uncertainty.
Re-centering on physiology.
Separating emotional urgency from medical urgency.
This is not psychotherapy.
It is consult cognition.
Difficult affect changes how danger is perceived.
Expert consultants learn to see that shift — and to compensate for it.
Why this matters for Consult Practice
Consult Practice is not only about what consultants think.
It is about where and how that thinking is made possible.
Rounding structures:
- shape Orientation
- constrain Thinking
- channel Execution
They teach trainees what counts as primary reality.
Recognizing this allows consultants to become intentional architects of their cognitive environment.
Not to impose a single best method.
But to understand that structure is not neutral.
How you round teaches what kind of doctor you are training.
It teaches what kind of judgment you are normalizing.
And once we recognize rounding as cognitive architecture, we gain the ability to design it with intention rather than inheritance.
Over time, that design quietly determines what kind of medicine an institution becomes.