Why temperature has always mattered more than we admit
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Cold has never been neutral to blood.
Long before hemoglobin was named or circulation mapped, physicians, philosophers, and lay observers recognized that cold altered the character of blood, how it flowed, how it thickened, how life seemed to retreat from the periphery toward the core. Across cultures and centuries, cold was understood not merely as an external condition, but as a force that slowed vitality, impaired cohesion, and threatened distribution.
Cold agglutinin disease sits squarely within this long intellectual lineage. It is modern in mechanism, but ancient in intuition.1
Blood as a living fluid
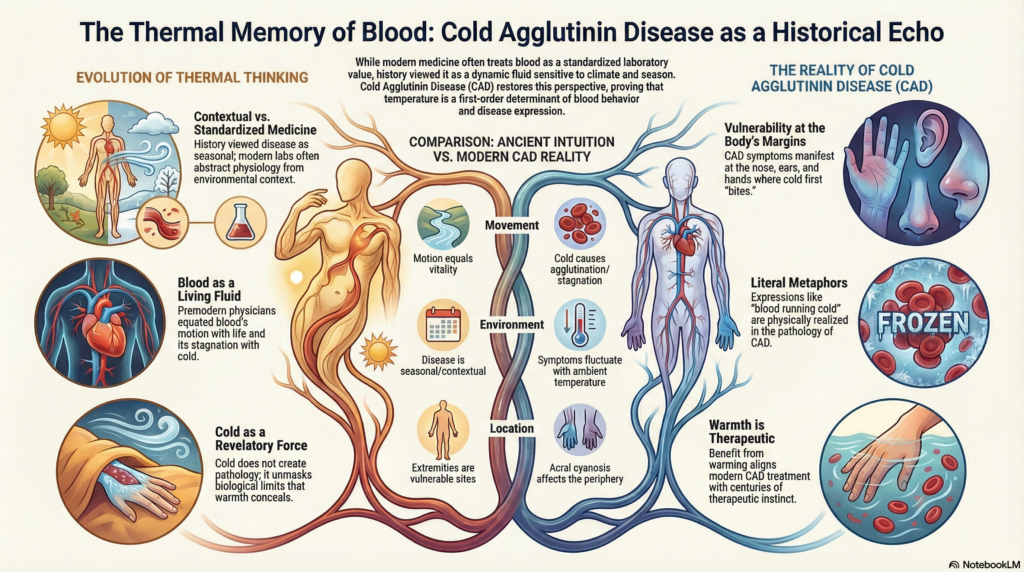
For most of medical history, blood was not conceived as a suspension of cells in plasma. It was understood as a living, dynamic substance, sensitive to season, climate, and internal balance.2
In Hippocratic medicine, cold was associated with thickening, stagnation, and obstruction. Seasonal writings described winter illnesses marked by cold extremities, sluggish circulation, and pain attributed to congealed or slowed blood. Premodern physicians did not know the mechanism, but they recognized the pattern. Blood that failed to move freely was dangerous, not because of clot alone, but because motion itself was equated with life. In texts such as Airs, Waters, Places, climate and season were explicitly linked to bodily function and disease expression.
Galen extended this view, describing blood as something that must remain warm and mobile to nourish tissues properly. Cold, in this framework, impeded the body’s internal economy. It slowed distribution, dulled sensation, and produced visible changes at the body’s margins. Cyanosis, though unnamed, was observed.
What earlier medicine lacked in molecular explanation, it often compensated for in close attention to environment and variation.
Even without microscopes or rheology, clinicians recognized a simple truth:
Cold blood does not behave like warm blood.
Cold, periphery, and vulnerability
Across cultures, the body’s edges have always been considered vulnerable to cold.
Hands, feet, ears, and noses appear repeatedly in medical and cultural traditions as sites where cold “bites,” circulation weakens, and color changes betray internal imbalance. Medieval regimen texts advised protecting extremities to preserve vitality. Folk medicine emphasized warming hands and feet not for comfort, but for health.
The places earlier cultures marked as vulnerable in the cold are precisely where CAD declares itself first.
Cold as moral and environmental force
Historically, cold was not just physical. It carried moral and existential meaning.
Cold climates were associated with hardship, threat, and endurance. Warmth symbolized safety, sociability, and life. Medical thinking absorbed these associations. Cold was something to be resisted, buffered against, or mitigated through clothing, diet, and environment.
Importantly, cold was also understood as contextual. The same body behaved differently in winter than in summer. Disease was seasonal. Symptoms fluctuated. This worldview tolerated variability rather than demanding constancy.
Modern medicine, by contrast, often assumes that physiology should be stable across environments. CAD exposes that assumption.
The disappearance of temperature from modern thinking
As medicine became laboratory-driven, temperature receded as a general explanatory variable.
Blood tests are performed under standardized thermal conditions. Hemoglobin values are interpreted as absolute. Physiology is abstracted from climate, season, and place. Temperature becomes background, not mechanism.
Yet CAD restores temperature as a first-order determinant of blood behavior. Symptoms fluctuate with seasons, rooms, procedures, and climates. The disease cannot be fully understood without restoring temperature to the foreground.
In this sense, CAD is not exotic. It is anachronistic. It behaves like diseases once did, sensitive to context, environment, and flow.
Re-reading CAD through history
Seen through this lens, familiar features of CAD take on deeper coherence:
- acral cyanosis reflects ancient observations about cold and the body’s margins
- seasonal fluctuation echoes premodern acceptance of environmental physiology
- benefit of warming aligns with centuries of therapeutic instinct
- limited benefit from vasodilators reflects that the dominant problem is altered blood behavior rather than isolated vascular spasm
What CAD restores to medicine
Cold agglutinin disease returns several neglected ideas to clinical consciousness:
- blood is not inert, it is responsive
- environment shapes disease expression
- physiology is conditional, not absolute
- warmth is therapeutic, not merely comforting
These are not new insights. They are old ones, resurfacing with molecular specificity.
A disease that remembers what we forgot
CAD is a reminder that medicine once took climate, season, and temperature seriously, not as modifiers, but as determinants. It challenges the modern habit of treating numbers as universal truths detached from context.
In that way, CAD is not only a hematologic disorder.
It is a historical echo.
It remembers a time when blood was understood as something that must be kept warm to stay whole, and when cold was recognized as a force capable of undoing cohesion at the body’s edges.
Modern science explains how this happens.
History explains why it makes sense.
Key reflections
- temperature shapes interpretation — how humans understand blood clinically and culturally
- pattern preceded mechanism — earlier physicians observed correctly without molecular explanation
- precision can obscure context — modern measurement sometimes hides environmental physiology
- CAD reunites mechanism with environment — restoring temperature as a biologic variable
- disease reveals assumptions — illness exposes hidden premises in medical thinking
Cold agglutinin disease does not contradict medical history. It fulfills it.
Historical Perspective Note
Premodern physicians often overexplained disease through climate, season, and balance. Modern medicine sometimes underexplains them. CAD reminds us that temperature can be more than background context. It can be a biologic variable that determines when blood behaves normally and when it fails.
Reflect and Apply
When you next see a patient with cold-sensitive symptoms, ask yourself:
Are you interpreting laboratory values as if they were independent of season, place, and temperature?
Or are you restoring environment and context to the foreground?
That feels more directly connected to the essay.
Additional Reading
- Hippocrates – Airs, Waters, Places
- Modern “airs, waters, places” reception
- Hippocratic Aphorisms on cold
- General overview of humoral medicine
- Galen: Anatomy and Physiology
- Liu Y. et al. Chinese Herb and Formulas for Promoting Blood Circulation and Removing Blood Stasis and Antiplatelet Therapies. Evid Based Complement Alternat Med. 2012.