When vulnerability is specific, not global
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Medicine often treats fragility as a synonym for frailty.
It should not.
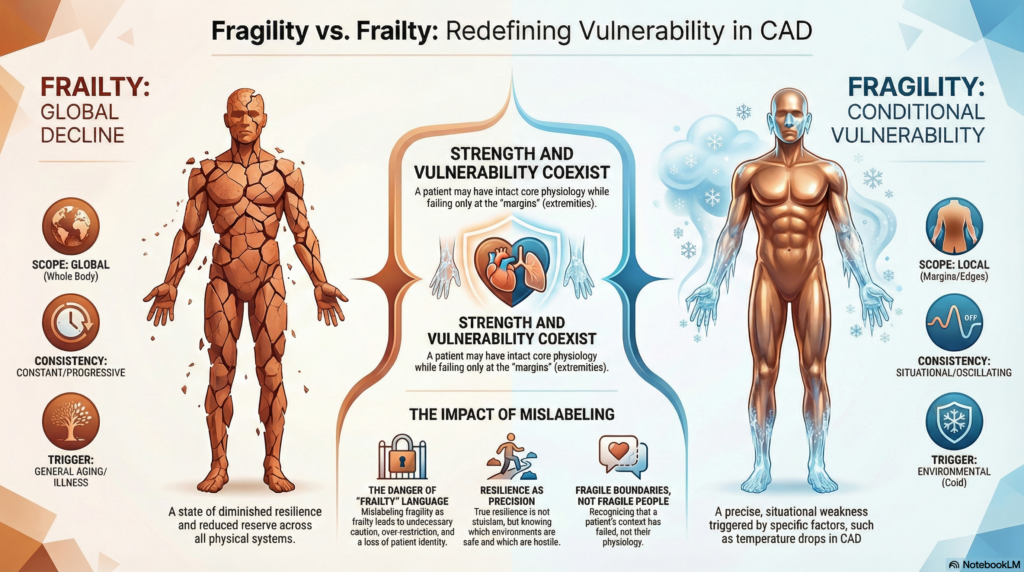
Frailty, in its formal clinical sense, refers to global decline: reduced reserve, diminished resilience, vulnerability across systems. It is measurable, multidomain, and persistent.
Fragility, by contrast, can be precise.
Local. Conditional. Activated only under certain circumstances.
Cold agglutinin disease makes this distinction visible.
A patient with CAD may walk miles, work full days, think clearly, and live independently. Their strength is intact. Their central physiology is competent. And yet, a drop in temperature can abruptly unmask vulnerability. Fingers discolor. Fatigue appears. Circulation falters. The margins fail.
This is not frailty.
It is fragility without general weakness.
Conditional vulnerability
Fragility in CAD is not constant. It is situational.
Warmth restores function. Cold withdraws it. The same body oscillates between capability and limitation without intrinsic decline. Vulnerability is not diffuse, and it is not progressive by default. It is conditional.
The physiologic boundary is real. Thermal sensitivity determines how wide that boundary is. Some patients are vulnerable only in deep cold. Others experience symptoms at modest temperature shifts. But in each case, the vulnerability is specific, not global.
This challenges a common clinical habit: equating vulnerability with deterioration.
It appears in notes that describe winter flares as “clinical worsening,” or in referrals that label otherwise independent patients as frail based solely on cold sensitivity. Informal frailty language creeps in long before formal frailty assessment would justify it.
A patient who becomes symptomatic in winter may be mistaken for declining, when in fact they are encountering a hostile environment.
Their physiology has not failed.
The context has.
The danger of mislabeling
When fragility is misread as frailty, consequences follow.
Patients may be counseled more cautiously than necessary. Activity may be discouraged rather than adapted. Independence may be quietly underestimated. Prognosis may be shaded darker than warranted.
The shift occurs not only in the chart, but in identity.
A person described as “frail” absorbs a global judgment. A person understood to have fragile boundaries retains strength everywhere else.
Frailty language flattens nuance. It converts conditional risk into assumed incapacity.
In CAD, that conversion is often wrong.
This does not mean fragility can never evolve into frailty. Deconditioning, cumulative avoidance, aging, or complications may alter the picture over time. But conditional vulnerability should not be prematurely treated as global decline. Expert care requires watching for transition, not assuming it from the outset.
Fragility at the margins
Cold agglutinin disease does not affect the body uniformly. It affects the periphery.
Some diseases do not weaken the center.
They destabilize the edges.
Hands, feet, ears, nose. Peripheral circulation. Seasonal participation. Social rhythm. These are the first domains affected. Core stamina and cognition often remain intact.
The width of the boundary varies. But the pattern is consistent: failure at the margins without collapse at the core.
Patients feel this immediately. Medicine sometimes misses it, because it looks first for global deterioration.
Rethinking resilience
Resilience is often defined as the ability to withstand stress. But for patients with conditional fragility, resilience is not endurance at all costs.
It is precision.
Knowing when protection is necessary and when it is not.
Knowing which environments are hostile and which are safe.
Knowing that vulnerability in one domain does not negate strength in others.
Avoiding cold is not weakness. It is accuracy.
Recognizing fragility without frailty allows clinicians to support that precision rather than undermine it.
Why this distinction matters
When clinicians recognize conditional fragility:
- vulnerability is not mistaken for decline
- adaptation is not confused with avoidance
- protection does not become over-restriction
- seasonal fluctuation is not labeled deterioration
- patients are not reduced to their worst month
Most importantly, patients remain whole.
They are not fragile people.
They are people with fragile boundaries.
Cold agglutinin disease reminds us that strength and vulnerability are not opposites. They often coexist in the same body, activated by context, not character.
Key reflections
- fragility is conditional — vulnerability may appear only under specific environmental stressors
- frailty is global — it implies persistent physiologic decline across domains
- mislabeling shapes care — calling fragility “frailty” can lead to unnecessary restriction and pessimistic prognosis
- strength and vulnerability coexist — patients may be robust centrally yet fragile at physiologic margins
- context reveals physiology — environment can unmask limits without changing underlying health
Reflect and Apply
Review a recent note for a patient with a chronic, environmentally sensitive condition.
Did your language describe a fragile person,
or a person with specific fragile boundaries?
What would change in your counseling, documentation, and expectations if you rewrote that distinction explicitly?