The following poll was posted on Twitter 1/13/24:
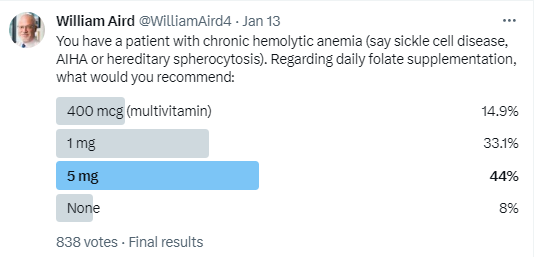
As you can see, the most popular answer was 5 mg/day.
There is little evidence to guide our decision here. Other than a single trial in children with sickle cell disease published in 1983, there have been no randomized studies exploring the risks-benefits or dose effects of folic acid supplements in hemolytic anemia.
Now that food is fortified with folate in most developing countries, folate deficiency is rare, and that is probably true even in those with increased RBC turnover from hemolytic anemia.
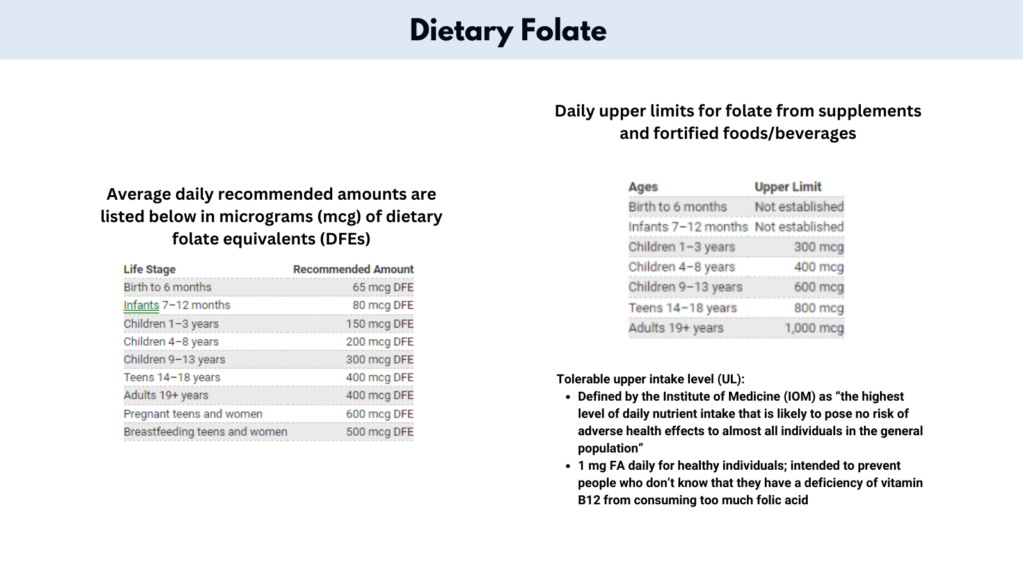
But, you may say, folic acid is just a vitamin. What’s the harm of giving a supplement to a patient with hemolytic anemia, just to err on the side of caution? And if we are going to give it, we may as well go all out and give 5 mg daily (5 x the daily upper limit).
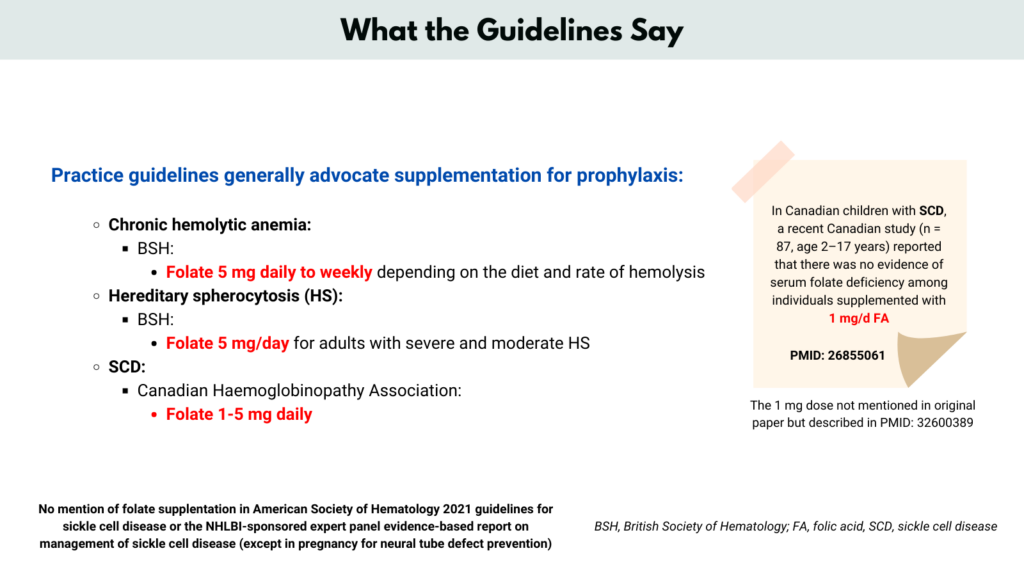
And you would find support in the few guidelines that mention folic acid supplementation in such patients.
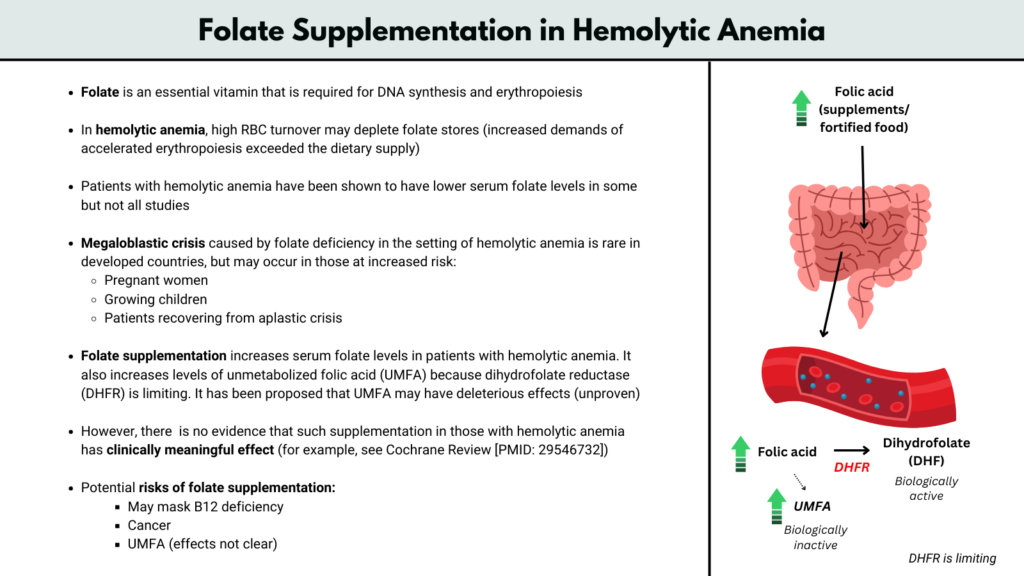
However, the potential downside of high doses of folic acid is that the resulting elevation in serum folate levels may mask the presentation of vitamin B12 deficiency.
Moreover, for folic acid to be biologically active, it must be converted in the body by dihydrofolate reductase (DHFR). Studies have shown that the latter enzyme is present in limited quantities.. Thus, high intake of folic acid results in high levels of unmetabolized folic acid (UMFA), which may have unwanted effects (such adverse effects remain to be proven).
At the end of the day, supplementation is probably preferred over no supplementation in patients with significant hemolytic anemia, and 1 mg/day is generally sufficient (possibly more during pregnancy and severe hemolysis/hemolytic crisis).
We need studies!!
See Cochrane review Folate supplementation in people with sickle cell disease.