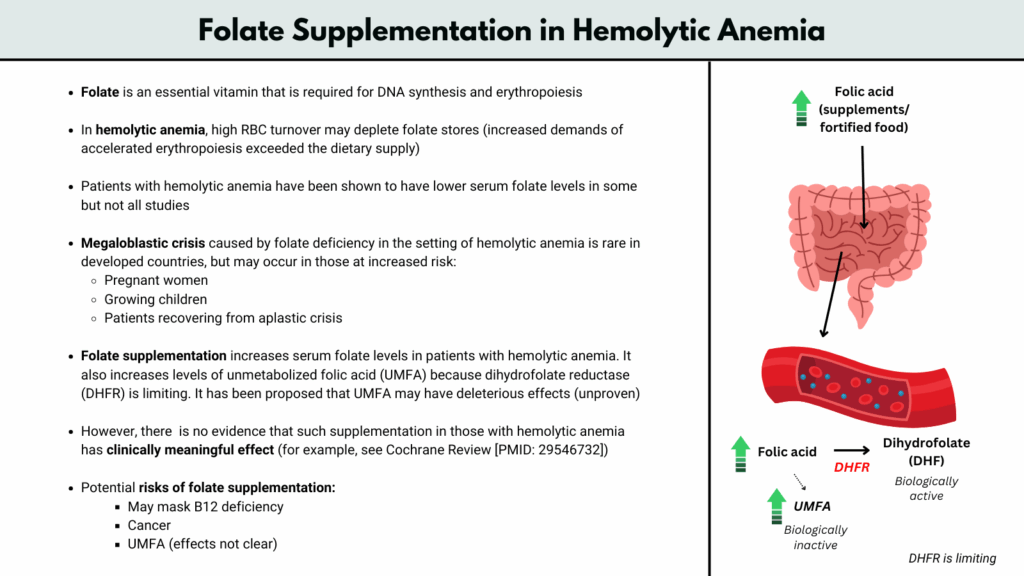
Folate is an essential vitamin required for DNA synthesis and erythropoiesis, and its demand increases significantly during accelerated red blood cell (RBC) production. In hemolytic anemias, where there is high RBC turnover, the bone marrow ramps up erythropoiesis to compensate, potentially leading to folate depletion if dietary intake cannot keep up with increased needs. Studies have shown that patients with hemolytic anemia may have lower serum folate levels, though findings are inconsistent across different populations. While megaloblastic crisis due to folate deficiency is rare in developed countries, it may occur in high-risk individuals such as pregnant women, growing children, or those recovering from an aplastic crisis. Folate supplementation reliably increases serum folate levels in these patients but also leads to accumulation of unmetabolized folic acid (UMFA) due to limited activity of the enzyme dihydrofolate reductase (DHFR), the implications of which remain uncertain. Although theoretically beneficial, there is no clear clinical evidence that folic acid supplementation meaningfully improves outcomes in hemolytic anemia, as noted in systematic reviews such as the Cochrane Review (PMID: 29546732). Furthermore, potential risks of routine supplementation include masking vitamin B12 deficiency, possible links to cancer promotion, and concerns about UMFA accumulation. Therefore, the decision to supplement should be individualized, particularly in patients with high physiologic demands or limited dietary intake.
For larger image, click here.
{kind=link}
Why folate matters in hemolytic anemia
- In hemolytic anemias, red blood cells are destroyed prematurely, which stimulates the bone marrow to ramp up red cell production (erythropoiesis) in compensation. This increased erythropoietic activity leads to accelerated utilization of folate, a vitamin essential for DNA synthesis and cell division, particularly in rapidly proliferating cells like erythroid precursors.
- Folate deficiency does not contribute to the hemolysis itself, but if folate becomes depleted, it can impair red cell production, worsening anemia and undermining the marrow’s compensatory response.
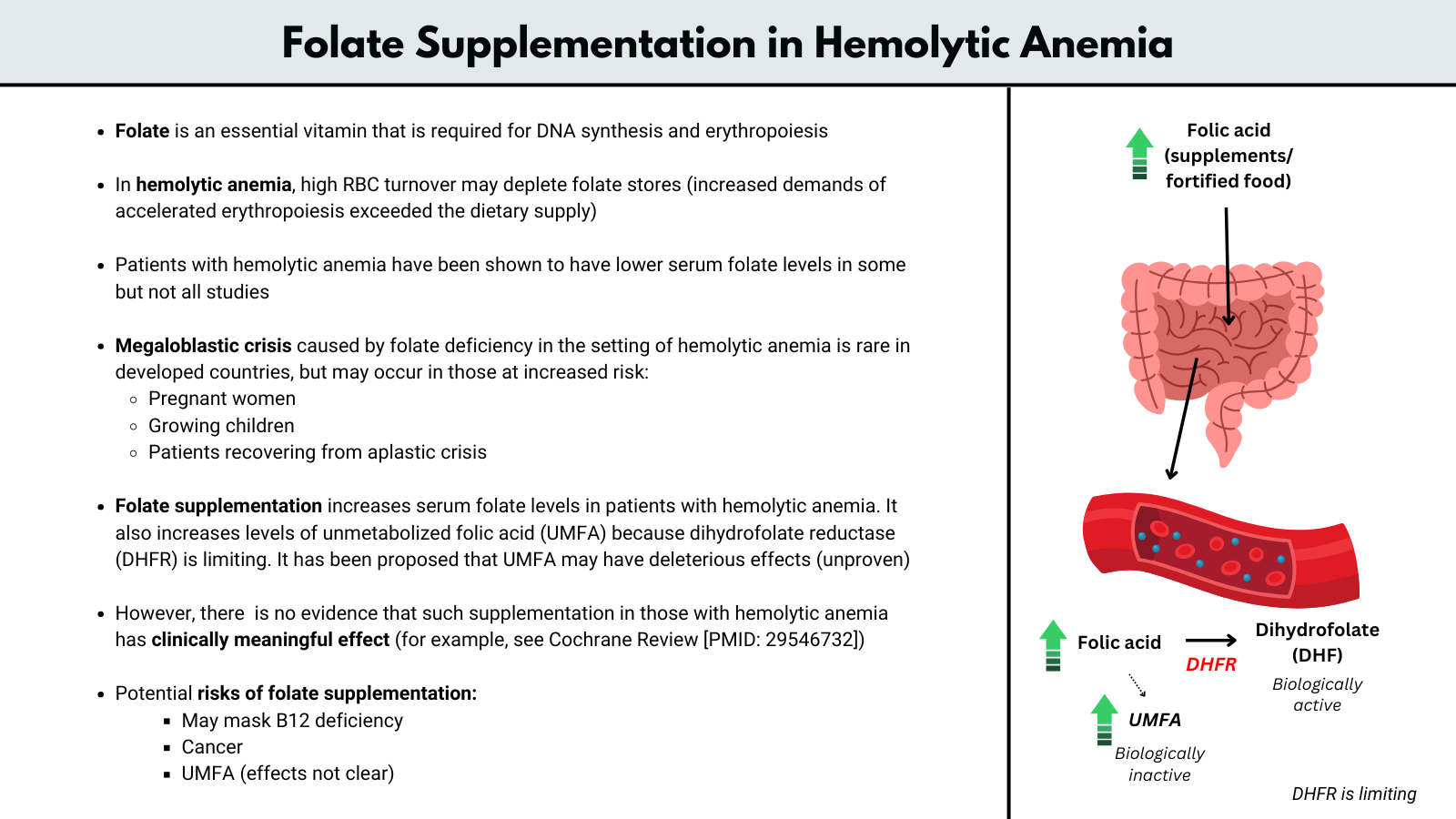
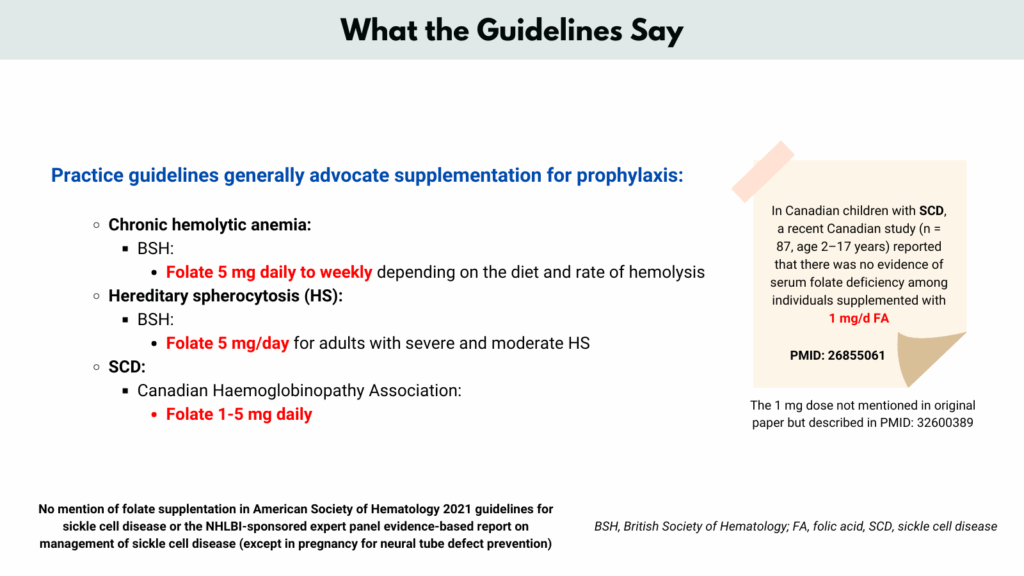
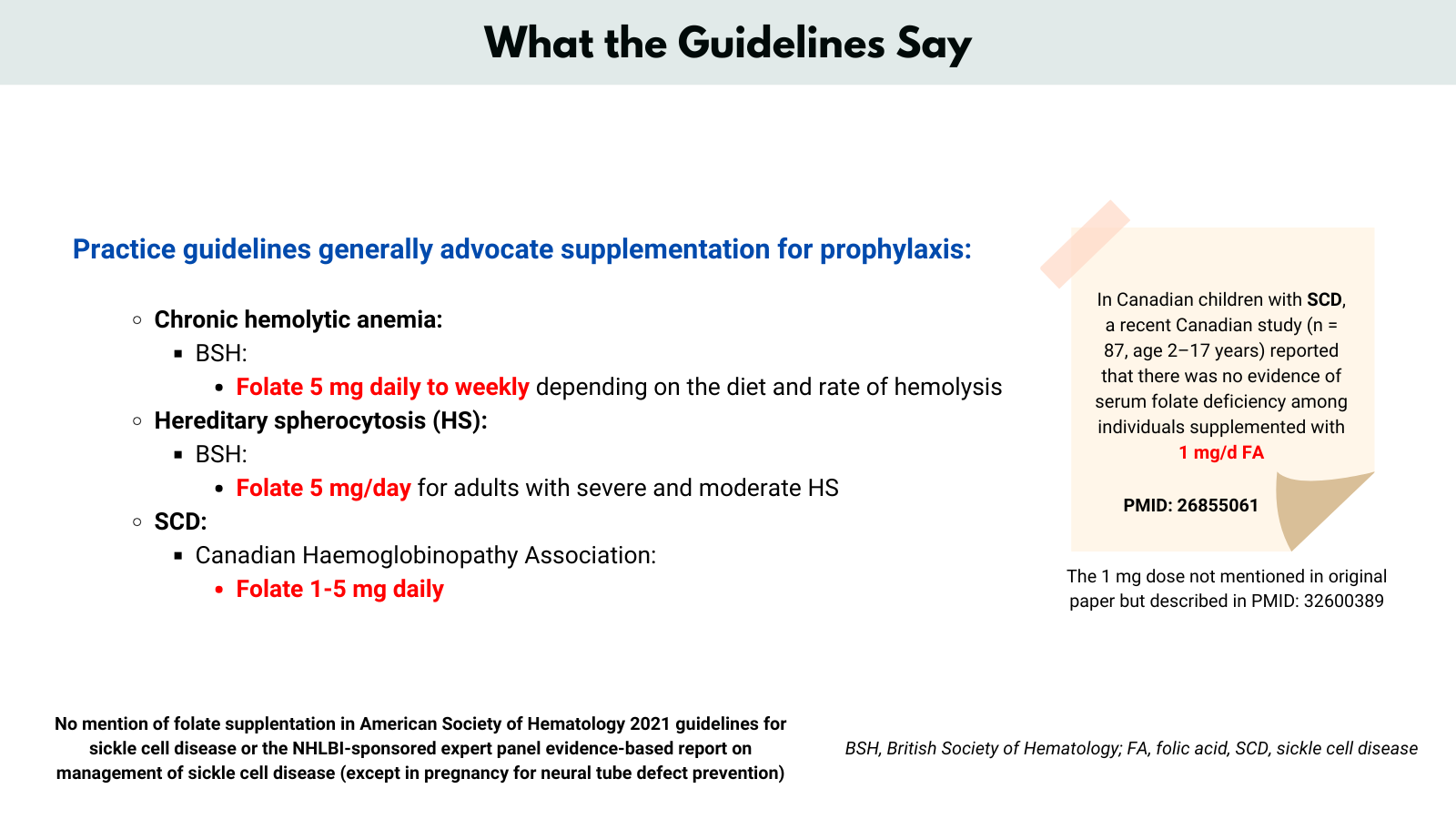
- There is limited high-quality evidence supporting this practice, but consensus guidelines and clinical experience endorse folic acid to prevent deficiency and support erythropoiesis.
- However, clinical folate deficiency is now rare even in chronic hemolytic disorders, partly due to food fortification and possibly excessive supplementation.
- Williams et al. Folic acid supplementation in children with sickle cell disease: a randomized double-blind noninferiority cross-over trial. Am J Clin Nutr. 2025 Apr;121(4):910-920.
- Background:
- Children with sickle cell disease (SCD) are routinely supplemented with 1–5 mg/d folic acid due to presumed increased requirements from chronic hemolysis and erythropoiesis. However, mandatory food fortification and advances such as hydroxyurea (which prolongs red blood cell lifespan) have raised questions about current supplementation practices.
- Study Design:
- Double-blind, randomized controlled cross-over trial (Canada).
- 31 children (ages 2–19) with SCD, most on hydroxyurea.
- Each participant received either 1 mg/day folic acid or placebo for ~12 weeks, then switched after a washout.
- Primary outcome: red blood cell (RBC) folate concentration.
- Secondary: serum folate, 1-carbon metabolites (total homocysteine, methylmalonic acid, vitamin B12, etc.), and clinical outcomes (acute pain episodes, megaloblastic changes).
- Results:
- RBC Folate: Supplementation with 1 mg folic acid/day led to significantly higher RBC folate than placebo (mean difference –179 nmol/L in intention-to-treat analysis), but the results were equivocal for confirming the noninferiority of placebo (CI crossed predefined noninferiority margin).
- Folate Deficiency: No participants developed serum folate deficiency (<7 nmol/L) during placebo period; a small number became RBC-folate deficient, but not serum-folate deficient.
- Clinical Outcomes: There were no significant differences between folic acid and placebo in hematological parameters, frequency of acute pain episodes, or occurrence of megaloblastic changes.
- 1-Carbon Metabolism: No significant changes in homocysteine, vitamin B12, methylmalonic acid, or other 1-carbon pathway markers between groups.
- Diet & Fortification: Dietary folate intake was substantial due to food fortification; most children maintained adequate folate status even during the placebo phase.
- Safety: Some individuals had detectable unmetabolized folic acid during supplementation, but no adverse clinical events attributable to folic acid or placebo.
- Conclusions:
- Folic acid supplementation (1 mg/day) significantly raises RBC and serum folate concentrations, but most children with SCD in a food-fortified country maintain adequate folate status even without supplementation. No evidence that supplementation with 1 mg/day translates to improved hematological or clinical outcomes over placebo within 12 weeks. The necessity and routine nature of prophylactic folic acid supplementation in this population may need to be re-examined, especially in the context of fortification and modern medical management.
- Background:
Key physiological points
- Folate is required for thymidine synthesis, a critical component of DNA.
- In folate deficiency, DNA synthesis becomes faulty, leading to megaloblastic changes in the bone marrow and ineffective erythropoiesis.
- This is especially problematic in settings of chronic or high-turnover hemolysis, such as:
- Sickle cell disease
- Hereditary spherocytosis
- Autoimmune hemolytic anemia
- G6PD deficiency (during active hemolysis)
Supplementation strategy
- Daily folic acid supplementation (typically 1 mg/day) is commonly recommended in patients with chronic hemolysis to prevent subclinical or overt deficiency.
- This is particularly important in pregnant patients, who have increased folate needs on top of any hemolytic condition.
- Several recent studies indicate that folic acid doses commonly prescribed (1–5mg daily) often lead to serum folate levels well above the normal range, suggesting that actual requirements might be lower, particularly in children with sickle cell disease or thalassemia.
- Most guidelines still prefer supplementation over no supplementation in significant hemolytic anemia, but emphasize the following points:
- 1 mg/day is adequate for most individuals.
- Higher doses (5 mg/day) are not routinely required and may result in unnecessary elevations in serum folate.
- Regular monitoring of serum folate, and awareness of vitamin B12 status, are recommended to balance benefits and risks, especially with long-term high-dose supplementation.
- Folic acid should not be used as a substitute for vitamin B12 therapy if deficiency is suspected, since folate can correct anemia while unmasking or worsening neurological complications from B12 deficiency.
- How do we arrive at 1 mg? Let’s work through some numbers:
- Dietary folate requirement (Recommended Dietary Allowance, RDA) ~400 mcg/day of dietary folate equivalents (DFE)
- This includes food folate + supplemental folic acid, with:
- 1 mcg food folate ≈ 1 DFE
- 0.6 mcg folic acid (with food) ≈ 1 DFE
- 0.5 mcg folic acid (empty stomach) ≈ 1 DFE
- Thus, ~200–400 mcg/day of absorbed folate is needed in a healthy adult to support baseline hematopoiesis and DNA synthesis.
- In hemolytic anemia, red cell turnover increases dramatically, which ramps up demand for DNA synthesis in erythroid precursors.
- The average lifespan of a red cell is ~120 days.
- In moderate to severe hemolysis, this may drop to 10–30 days.
- To compensate, erythropoiesis increases 3–8× baseline, depending on severity.
- This means:
- Folate requirement may increase 2–5 fold (or more in severe cases).
- So, folate needs can rise to ~1–2 mg/day, possibly higher in extreme hemolysis (e.g., sickle cell crisis, severe autoimmune hemolysis).
- Thus, 1 mg/day of folic acid is sufficient for most patients — 5 mg is rarely necessary, except in very specific circumstances.
- There is direct evidence indicating that 1mg of folic acid daily is generally sufficient and that higher doses (such as 5mg) often result in supraphysiological (overshoot) serum folate levels without demonstrated additional clinical benefit in patients with hemolytic anemia:
- Van der Dijs et al. Optimization of folic acid, vitamin B(12), and vitamin B(6) supplements in pediatric patients with sickle cell disease. Am J Hematol. 2002 Apr;69(4):239-46.
- Study design:
- 21 pediatric sickle cell disease (SCD) patients (ages 7–16, both HbSS and HbSC) underwent an 82-week dose-escalation study with stepwise increases in folic acid (400, 700, 1,000μg), vitamin B12 (1, 3, 5 RDA), and vitamin B6 (1, 3 RDA) supplementation.
- The functional marker for adequacy was plasma homocysteine, a sensitive measure of vitamin-dependent metabolic status.
- Main Findings (regarding folate):
- Plasma homocysteine levels dropped as folic acid was increased from 0 to 400 μg/day and from 400 to 700 μg/day but further increases from 700 μg (0.7 mg) to 1,000 μg (1 mg) did not significantly reduce homocysteine any further, indicating no added functional benefit above 700 μg.
- A practical daily regimen of 1 mg folic acid (which is easily achieved with standard supplements) is effective and likely covers the needs of nearly all pediatric SCD patients, considering some variability in dietary intake.
- Raising folic acid supplementation above 1 mg/day does not yield further biochemical (homocysteine-lowering) benefits, supporting that higher doses are unnecessary and could lead to unnecessary “overshoot” (supraphysiologic body folate levels).
- Clinical Recommendation:
- Optimal Supplementation: For pediatric SCD patients, 1mg of folic acid per day is both adequate and practical. Higher doses do not confer extra benefit and may lead to excessively high folate levels.
- Study design:
- Azzam M and Attalla. Serum Folate Levels in Patients with Chronic Hemolytic Anemia on Regular Folic Acid Supplementation Before and After Dose Modification. Indian Pediatr. 2019 Oct 15;56(10):845-848.
- Background: Folic acid supplementation is routine for patients with chronic hemolytic anemia (such as sickle cell disease and thalassemia), based on increased requirements due to chronic red blood cell breakdown. However, the actual needed dose and impact on serum folate levels are unclear.
- Design:
- Phase 1: Cross-sectional analysis of 134 pediatric patients (mostly sickle cell, some thalassemia) taking varying folic acid doses (mostly 1 mg, 2 mg, or 5 mg daily). Serum folate levels were measured.
- Phase 2: After high initial results, all patients (n=148) were switched to 1 mg/day for six months and retested.
- Findings:
- Phase 1
- 93.2% of patients had serum folate above the upper limit of the normal range (mean 77 nmol/L).
- Higher dosages correlated with even higher serum folate.
- Phase 2
- After standardizing to 1mg/day, 42.5% of patients still had serum folate above the upper limit, but levels were lower than in Phase 1 (mean serum folate 42.4nmol/L).
- All non-compliant patients (not taking folate) had normal values.
- No patient had sub-therapeutic folate values on 1mg/day.
- No significant differences in folate requirements by sex, but regularly transfused patients had higher serum folate.
- Vitamin B12 status remained normal for all.
- Phase 1
- Discussion & Implications:
- Even a standard dose of 1mg/day often raises serum folate above normal.
- Higher folate doses (such as 5mg) result in unnecessarily high serum concentrations, with no evidence of clinical benefit and potential risks (including masking B12 deficiency and other possible health concerns).
- Some people may not even require supplementation, as noncompliant patients had normal serum values.
- The study calls for re-evaluation of folic acid dosing in chronic hemolytic anemia and suggests routine monitoring of serum folate to balance benefit and potential harm.
- The findings support global trends suggesting that folic acid requirements in this population may be overestimated.
- Conclusion:
- Current folic acid doses (even as low as 1mg/day) for children with chronic hemolytic anemia are more than sufficient, and higher doses lead to excessive blood folate levels without added benefit. There is a strong call for individualized monitoring and perhaps even lower dosing in the future.
- Van der Dijs et al. Optimization of folic acid, vitamin B(12), and vitamin B(6) supplements in pediatric patients with sickle cell disease. Am J Hematol. 2002 Apr;69(4):239-46.
For larger image, click here.
{kind=link}
Clinical caveat
- While folate supplementation is important in hemolysis, it should not mask a concurrent vitamin B12 deficiency, which can also present with megaloblastic anemia but has different neurologic implications.
- Routine folate testing is often not reliable due to fluctuations from recent dietary intake, so prophylactic supplementation is usually favored in high-risk patients rather than relying on lab monitoring.
Conclusion
- Folate supplementation in hemolytic anemia supports the marrow’s response to increased red cell turnover. Without it, even the best-compensated hemolysis can become an underproduction problem. It’s a small intervention that protects against a big bottleneck in erythropoiesis.
- OpenEvidence:
- Folate supplementation is indicated in the setting of hemolysis when there is increased erythropoietic demand, as chronic hemolysis accelerates red cell turnover and depletes folate stores, predisposing to folate deficiency and megaloblastic anemia.
- Routine folate supplementation is not universally required in all hemolytic conditions but should be considered in patients with evidence of deficiency or in populations at high risk for deficiency due to chronic hemolysis.