How laboratory patterns, temperature, complement, and clonality converge
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
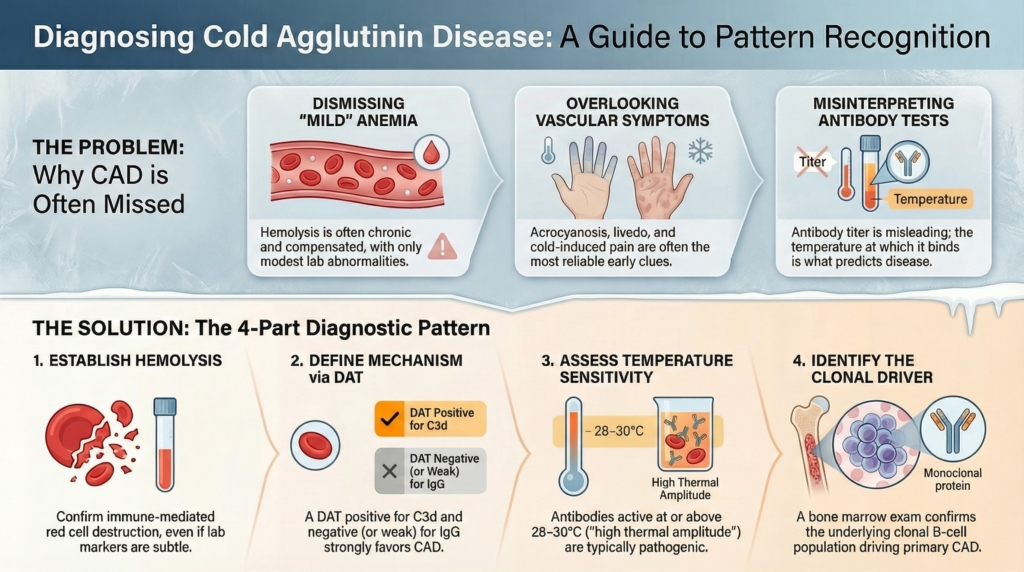
Diagnosis of cold agglutinin disease (CAD) is not established by a single test. It emerges from a pattern. Hemolysis may be incomplete, antibody titers misleading, and symptoms disproportionate to laboratory abnormalities. Accurate diagnosis requires integrating evidence of hemolysis, the DAT/complement pattern, temperature-dependent antibody behavior, and evaluation for an underlying clonal B-cell process.1
The first question is not ‘Is there a cold antibody?’ but ‘Is there clinically relevant hemolysis, and what is driving it?’
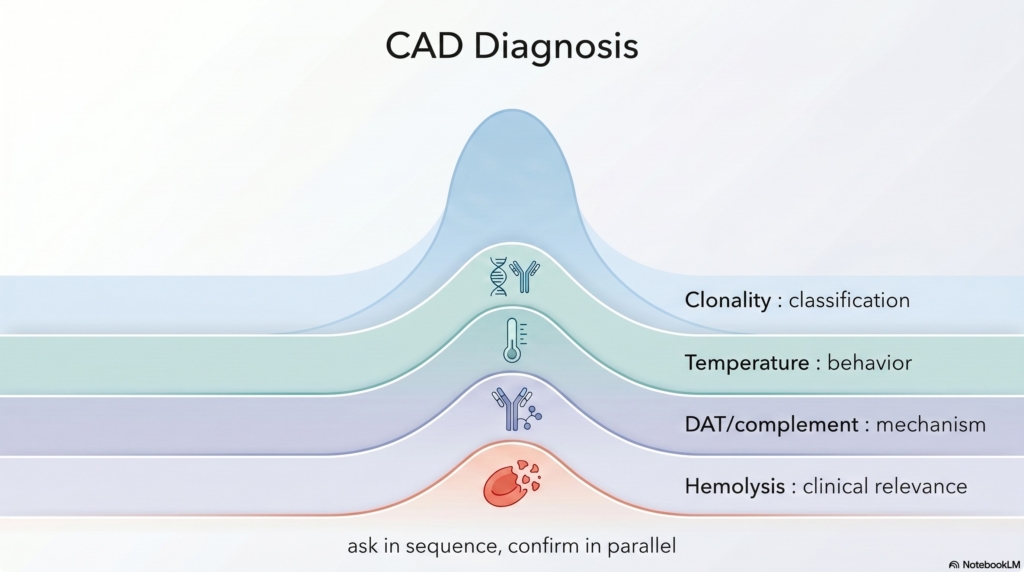
Each domain answers a different question: hemolysis establishes clinical relevance, the DAT/complement pattern supports mechanism, temperature explains behavior, and clonality informs chronicity and classification. In practice, these domains are applied sequentially.
For example, a patient with fatigue, mild anemia, and cold-induced finger discoloration might first be confirmed to have clinically relevant hemolysis, then shown to have complement-positive DAT, then demonstrated to have temperature-dependent antibody activity, and only afterward evaluated for a clonal B-cell population. The diagnosis emerges as each layer aligns.
Recognizing hemolysis — often incomplete, often underestimated
Hemolysis in CAD is frequently chronic, compensated, and laboratory-subtle, leading to underrecognition when clinicians expect dramatic biochemical abnormalities.2
Symptoms may not correlate closely with hemoglobin level alone and can reflect cold-induced circulatory disturbance in addition to anemia.3 For that reason, the hemolysis pattern in CAD is often best recognized by combining clinical context (symptoms and signs) with laboratory evidence, rather than expecting a dramatic biochemical signature in isolation.4
Typical laboratory features include:5
- anemia that is often mild to moderate rather than profound
- LDH and indirect bilirubin that may be only modestly elevated
- haptoglobin that may be low or borderline rather than absent
- reticulocyte responses that are variable and sometimes blunted
Fatigue and functional limitation may be disproportionate to the degree of anemia. In diagnosis, this should raise suspicion, but it should not replace objective evidence of hemolysis.6
The direct antiglobulin test (DAT): the diagnostic pivot
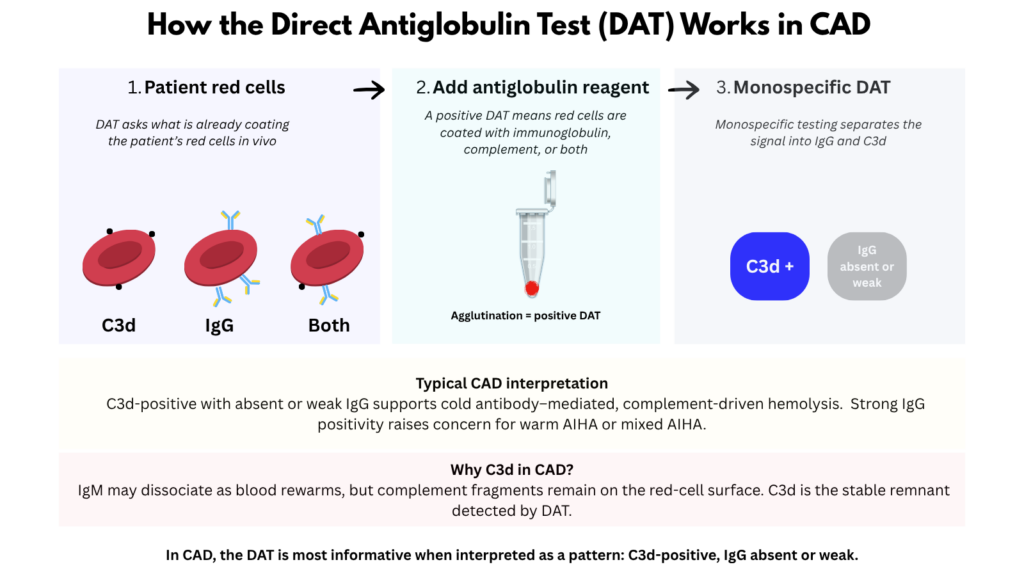
In CAD, the DAT pattern is more informative than DAT positivity alone. When CAD is suspected, monospecific DAT testing should be requested because polyspecific DAT alone cannot distinguish complement-mediated hemolysis from IgG-mediated disease.
In typical CAD, the DAT pattern is dominated by complement deposition, supporting a cold-antibody mechanism and helping distinguish CAD from warm IgG-mediated autoimmune hemolytic anemia.7
In CAD, complement is typically detected as C3d because C3b deposited on the red cell surface is progressively cleaved during circulation, leaving C3d as the stable remnant on surviving cells. This helps explain how DAT findings can remain strongly complement-positive even when hemolysis is chronic and partially compensated.8
Typical features include:9
- DAT positivity for C3d
- IgG that is usually negative or only weakly positive
Isolated C3d positivity in the appropriate clinical context strongly supports CAD.
By contrast, mixed DAT patterns require careful interpretation. True IgG plus C3 positivity raises the possibility of mixed autoimmune hemolytic anemia, which carries different diagnostic and therapeutic implications.10
Complement studies can provide supportive evidence of ongoing classical pathway activation. Low C4, sometimes with less marked reduction in C3, is compatible with classical pathway consumption in CAD, but these findings are supportive rather than diagnostic.11
Cold agglutinins: presence is not disease
Cold agglutinins are common in the general population, particularly at low titers. CAD should not be diagnosed based on their presence alone. Clinical relevance depends on antibody behavior and downstream complement effects.12
Low-titer cold agglutinins are frequently incidental, and antibody titer alone does not define pathogenicity. Although titers above traditional thresholds (for example, >1:64 at 4°C) are often reported as “significant,” this remains an imperfect surrogate for clinical relevance because temperature dependence and complement engagement matter more than quantity.13
Clinically significant CAD usually involves monoclonal IgM, with antibody activity at physiologic temperatures playing a dominant role.14
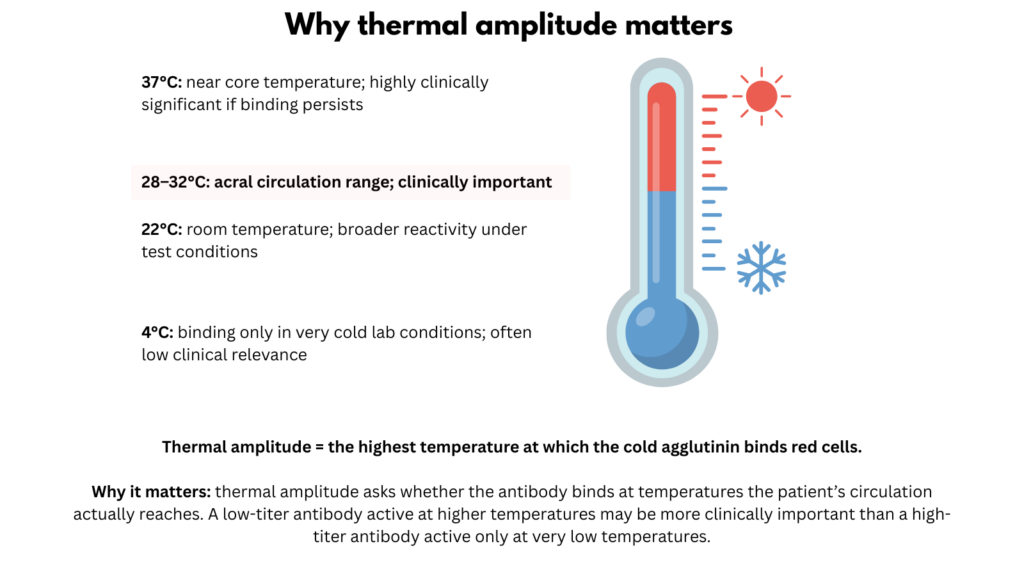
Thermal amplitude: the most underused diagnostic concept
Thermal amplitude, the highest temperature at which the antibody binds red cells, is a major determinant of clinical significance and generally correlates better with pathogenicity than titer alone. It explains seasonal variability, persistence of symptoms after cold exposure, and poor correlation between antibody titer and disease severity.15
Antibodies active near core body temperature are typically pathogenic and correlate with greater hemolysis and symptom burden.16 The reason is anatomical: higher thermal amplitude means IgM binding persists at temperatures encountered beyond the periphery, expanding the zone where complement can be activated and making hemolysis less dependent on extreme cold exposure alone.17
A low-titer antibody active at higher temperatures may cause more severe disease than a high-titer antibody binding only at low temperatures, explaining why antibody quantity alone is misleading.18
When thermal amplitude testing is unavailable, clinical behavior serves as a surrogate, including persistence beyond winter months or symptoms triggered by mild cold exposure.19
Distinguishing primary CAD from secondary cold agglutinin syndrome
This distinction alters diagnostic evaluation, prognosis, and management. Primary CAD is a chronic clonal disorder; secondary cold agglutinin syndromes occur in association with another condition, such as infection, autoimmune disease, or overt lymphoma.20
Primary CAD is characterized by:21
- chronic course
- clonal bone marrow B-cell disorder
- persistent complement-mediated hemolysis
Secondary cold agglutinin syndromes are associated with infection, autoimmune disease, or overt lymphoma and often resolve with treatment of the underlying condition.22
Infection may also unmask previously subclinical primary CAD, so longitudinal follow-up is often required to distinguish persistent clonal disease from self-limited post-infectious hemolysis.
When available, antibody specificity can also support classification. Infection-associated cold agglutinin syndromes are often polyclonal and may show anti-I specificity with Mycoplasma pneumoniae, whereas EBV-associated cases may show anti-i specificity, reinforcing that “post-infectious” disease is biologically heterogeneous.23
Bone marrow evaluation: diagnosing the clone
Bone marrow examination in cold agglutinin disease is performed to identify the antibody-producing B-cell clone, rather than primarily to assess tumor burden or nodal disease.24
Clonal B-cell populations are present in most patients with primary CAD. These clones are typically low-grade, indolent, and confined to the bone marrow rather than presenting as overt lymphadenopathy.25
Marrow involvement is often subtle and may be missed without careful histologic, immunophenotypic, and molecular evaluation. Flow cytometry is particularly useful because light-chain restriction and characteristic surface marker patterns can identify small clonal B-cell populations that are not evident morphologically.26
When present, the clonal population most often shows a marrow-based indolent B-cell lymphoproliferation that often does not fit neatly into classic lymphoma categories, supporting the concept that primary CAD is driven by a distinct marrow-based lymphoproliferative process rather than classic nodal lymphoma.27
Overt lymphoma is uncommon at the time of CAD diagnosis. The absence of radiographic lymphadenopathy or bulky disease should not be interpreted as evidence against primary CAD.28
Clone size correlates poorly with anemia severity. Clinical phenotype is driven more by antibody characteristics and complement engagement than by the extent of marrow infiltration. This disconnect explains why patients with minimal marrow disease may experience severe hemolysis, while others with larger clones remain relatively compensated.29
Bone marrow evaluation is recommended once CAD is suspected, but it does not always need to precede initial management. In patients with severe or rapidly progressive hemolysis, treatment may begin before full marrow characterization. In more stable patients, marrow evaluation helps clarify disease classification, informs prognosis, and guides longer-term management decisions.30
Diagnostic convergence in cold agglutinin disease
A diagnosis of primary CAD is strongly supported when the following signals align:
• clinically relevant hemolysis
• DAT pattern consistent with complement deposition (C3d ± weak IgG)
• cold antibody with clinically meaningful thermal amplitude
• monoclonal IgM with evidence of a marrow-based clonal B-cell population
No single finding is sufficient. Diagnosis emerges from convergence.
The same concept, visualized:
Even when these signals align, pre-analytical interference can obscure or distort laboratory interpretation.
Sample handling and laboratory interference: an invisible diagnostic pitfall
Cold agglutinins can interfere with routine blood counts if samples are allowed to cool before analysis. In some cases, visible clumping in the collection tube that resolves after warming is itself the first diagnostic clue. This pre-analytical issue can distort results and delay diagnosis. Specific artifacts include:31
- red cell agglutination may falsely lower RBC count
- MCV may appear spuriously elevated
- MCHC may be artifactually increased
- automated analyzers may flag clumping or report implausible indices
When CBC parameters appear internally inconsistent, warming the sample and repeating analysis is essential. Failure to recognize cold agglutinin interference can obscure hemolysis and mislead interpretation.32
Common diagnostic pitfalls
Diagnostic delay in cold agglutinin disease is usually conceptual rather than technical. Errors most often arise from misinterpreting patterns, underweighting symptoms, or applying inappropriate diagnostic frameworks.33
Common pitfalls include:34
- dismissing symptoms because anemia appears mild:
In CAD, fatigue, cold intolerance, pain, and functional limitation may be driven by complement activation and microvascular dysfunction rather than hemoglobin level alone. Symptom burden often exceeds what would be predicted by laboratory measures of anemia. - relying on cold agglutinin titer alone:
Cold agglutinin titers are an unreliable indicator of pathogenicity. Antibody behavior at physiologic temperatures and complement engagement are far more important determinants of clinical relevance than titer magnitude. - misclassifying CAD as warm autoimmune hemolytic anemia due to weak IgG DAT positivity:
Weak or borderline IgG positivity on DAT does not exclude CAD and may reflect nonspecific binding or technical factors. Interpretation should prioritize complement deposition and the overall clinical pattern. True IgG plus C3 positivity raises the possibility of mixed autoimmune hemolytic anemia, which requires different diagnostic and therapeutic reasoning. - assuming absence of overt lymphoma excludes CAD:
Most patients with primary CAD harbor a low-grade, marrow-based clonal B-cell disorder without bulky lymphadenopathy or radiographic evidence of lymphoma. Normal imaging does not rule out clonal disease. - failing to link cold exposure, seasonality, or environmental triggers to symptoms:
Disease activity that worsens with cold exposure, winter months, or air-conditioned environments provides an important diagnostic clue to temperature-dependent antibody activity and higher thermal amplitude.
Diagnosis as pattern recognition, not confirmation
CAD is diagnosed when multiple signals align: immune-mediated hemolysis, complement deposition on DAT, temperature-dependent IgM activity, and an underlying clonal B-cell disorder. No single test is sufficient. Sometimes the diagnosis converges in a single encounter, but often it requires longitudinal reassessment as persistence, temperature dependence, and clonality become clearer over time.35
Reflect and Apply
When you suspect CAD, resist the urge to ask, “Which single test proves the diagnosis?”
Instead ask:
Do the signals align?
Is there clinically relevant hemolysis?
Is the DAT pattern complement-dominant?
Is the antibody behavior temperature-dependent and clinically meaningful?
Is there evidence of a clonal or secondary disease context?
In CAD, diagnosis is not a yes-or-no laboratory event. It is a pattern that becomes convincing when mechanism, temperature, and clinical behavior point in the same direction.
Guideline perspective: diagnostic workup in suspected CAD
Consensus and guideline documents support the same convergence model. In suspected CAD, diagnostic evaluation should include:36
- objective assessment of hemolysis, including hemoglobin, LDH, bilirubin, haptoglobin, reticulocyte count, and peripheral smear review
- DAT testing with monospecific antisera, especially anti-C3d and anti-IgG
- cold agglutinin testing, including titer, with attention to specimen handling and clinical relevance
- assessment of thermal amplitude when the clinical significance of a cold antibody is uncertain37
- evaluation for a clonal B-cell disorder with serum protein electrophoresis, immunofixation, immunoglobulin studies, bone marrow biopsy, and flow cytometry
- distinction between primary CAD and secondary cold agglutinin syndrome
- baseline assessment for acrocyanosis or other cold-induced circulatory symptoms
- consideration of mixed AIHA when DAT shows both IgG and C3 positivity and the clinical picture suggests overlapping warm and cold mechanisms
- consideration of Donath–Landsteiner testing when the presentation suggests paroxysmal cold hemoglobinuria, especially with hemoglobinuria, atypical serology, or pediatric/post-infectious disease
These recommendations reinforce the core principle: CAD is diagnosed by aligned evidence of hemolysis, complement-pattern DAT findings, clinically meaningful cold antibody behavior, and clonal or secondary disease context.
Test your thinking
A short, judgment-focused quiz on the diagnosis of cold agglutinin disease.