Clinical Vignettes
Imagine you’re listening to case presentations on rounds:
- Case 1: A resident presents a patient with a platelet count of 149,000/µL and casually describes it as mild thrombocytopenia. Most of us wouldn’t quibble—149 feels mild.
- Case 2: Later, an intern presents a patient with a platelet count of 60,000/µL, introducing it as severe thrombocytopenia. Another intern overhears and pushes back: “That doesn’t sound severe to me—I’d only call it severe if the platelet count was below 20,000.”
- Case 3: In a different setting, a patient with end-stage renal disease is presented with a hemoglobin of 7.8 g/dL. The speaker calls this moderate anemia: “After all, the patient is comfortable, not symptomatic, and doesn’t need a transfusion.”
These vignettes highlight the problem:
- We often use terms like mild, moderate, or severe without a clear framework.
- Sometimes we’re implicitly relying on numerical thresholds.
- Other times, on clinical context.
- What sounds severe in one situation may feel moderate—or even mild—in another.
- And what sounds severe to one individual may feel moderate to another.
Framing the question
So how should we define severity?
- By strict laboratory cutoffs?
- Always in the context of the patient’s clinical state?
- Or simply at the mercy of whoever is presenting the case?
Teaching Point
The preferred answer, despite its imperfections. is to stick with agreed-upon definitions, warts and all.1
- They may be arbitrary.
- They may not fit every patient.
- And we may not always agree with them.
But definitions provide:
- A common language for communication.
- A framework for teaching and learning.
- Consistency in research and guidelines.
- A baseline for clinical decision-making.
Let’s come back to the case of the patient with end-stage renal disease and a hemoglobin of 7.8 g/dL. Yes, that is perfectly reasonable for someone in this clinical state. Such patients are physiologically adapted, with increased 2,3-DPG, and are rarely symptomatic at this level of hemoglobin.
But here’s the problem: when a speaker refers to a hemoglobin in a case like this without giving the actual number and simply states that it is moderate, or someone else says it is severe. which one is correct? According to the WHO definitions of anemia severity, 7.8 g/dL is severe.
The point is this: while clinical context is clearly important, relying on a speaker’s interpretation of severity is extremely subjective. It is impossible to get into the head of the presenter to know what they mean by “moderate” or “severe,” and their interpretation may not match yours.
By contrast, when we use strict definitions, we all know exactly what is being conveyed. If the speaker says severe anemia, I know that maps to a hemoglobin of less than 8 g/dL, whether or not that threshold feels clinically relevant in the moment. The severity maps to a number, and that shared understanding is what matters.
Thresholds for Severity
Anemia
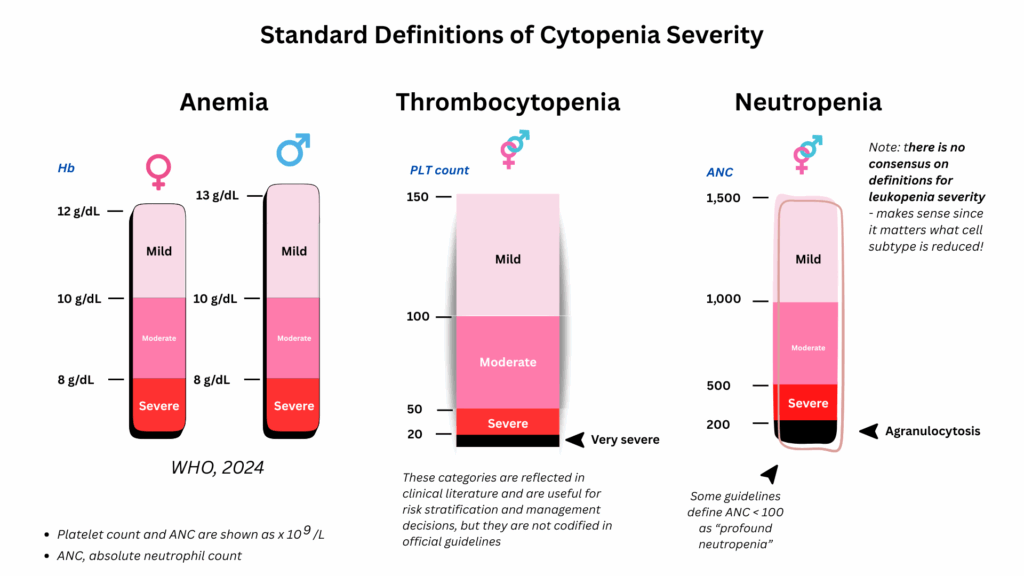
The World Health Organization (WHO) provides widely used thresholds for mild, moderate, and severe anemia, primarily for global surveillance and research purposes. In addition, oncology groups such as the National Comprehensive Cancer Network (NCCN) and other cancer associations have adopted similar grading systems for use in clinical trials and supportive care guidelines. While these cutoffs are somewhat arbitrary (they were chosen largely for population surveillance and research comparability) and do not always reflect clinical adaptation in individual patients, they serve as a standardized framework that allows us to speak the same language.
- World Health Organization (WHO):
- Non-pregnant women (≥15 years)
- Mild: 11.0 – 11.9 g/dL
- Moderate: 8.0 – 10.9 g/dL
- Severe: < 8.0 g/dL
- Men (≥15 years)
- Mild: 11.0 – 12.9 g/dL
- Moderate: 8.0 – 10.9 g/dL
- Severe: < 8.0 g/dL
- Comments:
- “The management for individuals with mild, moderate, or severe anaemia could vary depending on the clinical scenario and the underlying cause(s) of the anaemia.”
- “A clear association between severity of anaemia with clinical or statistical outcomes could be of great value for classifying anaemia severity at clinical/individual level and would help to prevent and treat anaemia.”
- Non-pregnant women (≥15 years)
Thrombocytopenia
Unlike anemia, there is no WHO classification of severity for thrombocytopenia. The scheme used here (mild, moderate, severe, very severe) comes from standard hematology textbooks and review articles. Severity thresholds for thrombocytopenia, commonly used in hematology (mild, moderate, severe, very severe), while not formally codified by WHO, are grounded in physiology and bleeding risk. Counts <20 ×10⁹/L, for example, consistently correlate with a higher risk of spontaneous bleeding. Thus, while these cutoffs are still consensus-based, they have a stronger empirical link to clinical outcomes than the anemia cutoffs.
- Mild: 100,000 – 149,000/µL
- Moderate: 50,000 – 99,000/µL
- Severe: 20,000 – 49,000/µL
- Very severe: < 20,000/µL
Leukopenia
Unlike anemia and thrombocytopenia, there are no widely accepted thresholds for grading the severity of leukopenia. This is because the total white blood cell count is a composite measure that includes five distinct subtypes: neutrophils, lymphocytes, monocytes, eosinophils, and basophils. The clinical significance of a reduced white cell count depends entirely on which lineage is affected. For example, neutropenia carries a clear risk of infection at defined thresholds, whereas isolated lymphopenia or monocytopenia has very different implications. In this sense, “leukopenia” is too generalized a concept to be meaningfully classified by severity without reference to the specific cell line involved.
- Neutropenia (absolute neutrophil count, ANC):
- Most clinically relevant “low count” definition because of infection risk.
- Common severity criteria (widely used in hematology, oncology, ID):
- Mild: ANC 1.0 – 1.5 ×10⁹/L
- Moderate: ANC 0.5 – 0.9 ×10⁹/L
- Severe: ANC < 0.5 ×10⁹/L
- Very severe / profound (agranulocytosis): ANC < 0.2 ×10⁹/L
- These thresholds are clinically grounded, since the risk of bacterial/fungal infection rises sharply below 0.5, and especially below 0.2.
- Lymphopenia (absolute lymphocyte count, ALC):
- Defined as ALC < 1.0 ×10⁹/L in adults.
- No universally standardized severity grading like neutropenia, but some references (e.g., HIV/AIDS staging) use:
- Mild: 0.8 – 1.0 ×10⁹/L
- Moderate: 0.5 – 0.8 ×10⁹/L
- Severe: < 0.5 ×10⁹/L
- Risk depends on context (e.g., HIV, chemotherapy, congenital immunodeficiency).
- Monocytopenia:
- Sometimes defined as absolute monocyte count < 0.2 ×10⁹/L.
- No recognized severity grading.
- Clinical relevance: usually not significant in isolation, but may appear in certain conditions (aplastic anemia, hairy cell leukemia, chemotherapy).
- Eosinopenia:
- Defined as absolute eosinophil count < 0.05 ×10⁹/L in some labs.
- No clinical grading system — low eosinophils are common and usually not clinically important (seen in stress, steroid therapy, sepsis).
- Basopenia:
- “Low basophils” is not recognized as a pathologic entity.
- Basophils are normally so few in number that even “zero” on a differential is within normal limits.
- No definition or severity scheme exists.
Of the five white cell subtypes, only neutropenia has well-defined severity criteria that directly correlate with infection risk. Lymphopenia is clinically important but lacks standardized severity grading outside of disease-specific contexts (e.g., HIV). Monocytopenia and eosinopenia may be defined but are rarely graded, and basopenia has no clinical relevance at all. Thus, the concept of “leukopenia severity” is meaningful only when broken down by lineage, with neutropenia as the paradigm.
Final Thoughts
The Challenge of Defining Severity
Ideally, severity definitions would map onto specific conditions and clinical realities.
- For example:
- In sickle cell disease, a hemoglobin of 8 g/dL may be “normal” for the patient and not clinically severe.
- In CKD or MDS, patients can be well-adapted at levels that WHO would classify as severe.
- In someone with a normal baseline hemoglobin three months ago, that same hemoglobin may reflect a rapid decline and be much more alarming.
Another approach could be to define severity based on symptoms or the need for intervention, for example, whether the patient requires transfusion.
But the more granular and context-specific the definitions become, the further we drift from consensus and standardization. And once that happens, the definitions lose their greatest utility: a shared language across clinicians, researchers, and public health professionals.
Thus, there is no clear “happy medium.” Definitions are always a compromise:
- Too rigid, and they ignore clinical reality.
- Too contextualized, and they lose reproducibility and usefulness.
Teaching point:
Severity grading is ultimately a balance. It provides a framework for communication, but it will never perfectly capture the diversity of patient experiences across different diseases. That tension is exactly why we need to both know the definitions and interpret them in clinical context.