Making expert judgment visible
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
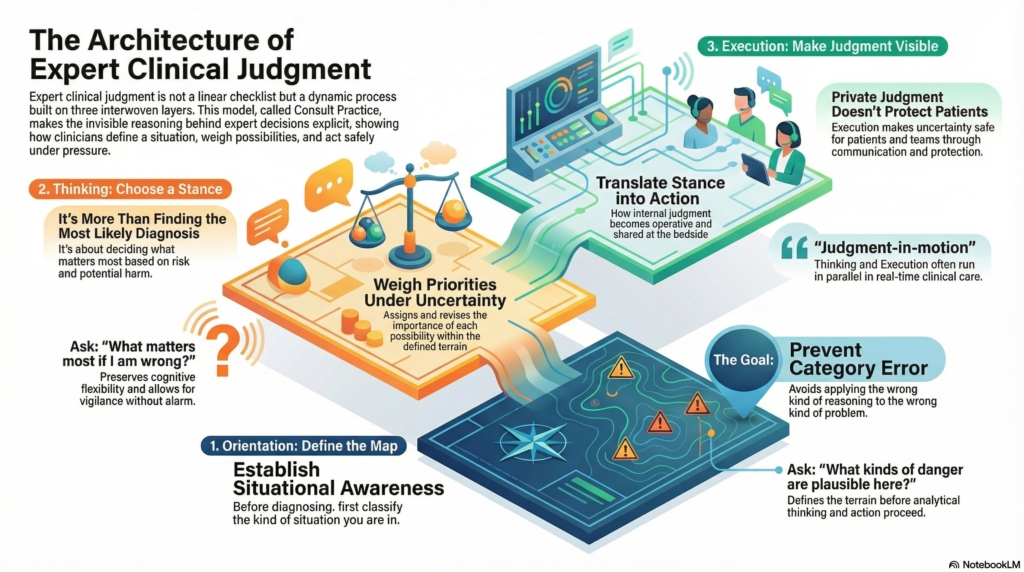
Consult Practice is built around three interlocking forms of expert clinical judgment:
- Orientation
- Thinking
- Execution
These are not steps in a checklist.
They are distinct cognitive functions that operate continuously during real clinical care.
Conceptually, judgment forms in this order:
Orientation → Thinking → Execution
In practice, however, these layers are temporally interwoven. Consultants think while they are executing. They execute while they are still thinking. They re-orient as new information and the consequences of their actions reshape the terrain.
Most clinicians are exposed first to Execution—orders, recommendations, notes, and visible actions—without seeing the Orientation and Thinking that made those actions safe.
Consult Practice works backward to make that invisible reasoning explicit.
It is designed to make expert judgment visible: not just what consultants do, but how they decide what kind of situation they are in, what matters most within that situation, and how that stance becomes shared, timed, and protective at the bedside.
The Three Layers of Consult Judgment
Think of Consult Practice as three nested layers of expert work:
Orientation = Defining the map
Thinking = Choosing a stance within that map
Execution = Making that stance visible and operative
They are not steps.
They are different kinds of cognitive and behavioral work.
They are conceptually ordered but temporally interwoven.
Orientation defines the terrain.
Thinking determines stance within that terrain.
Execution makes that stance visible through action and communication.
Execution is where judgment becomes shared, timed, and protective.
It is not a checklist.
It is judgment in motion.
Orientation, Thinking, and Execution — What Each Actually Does
Orientation
Orientation establishes situational awareness and defines the problem space.
It answers questions such as:
- What kinds of danger are plausible here?
- How urgent is this moment?
- How broad or narrow is the terrain?
- How much uncertainty can safely be tolerated?
- Is this a fast-moving, high-risk situation or a contained, watchful one?
Orientation does not diagnose.
Orientation does not instruct.
Orientation classifies the kind of situation you are in so that the right kind of thinking and execution become possible.
Orientation exists to prevent category error: applying the wrong kind of reasoning to the wrong kind of problem.
Premature commitment is one form of category error.
So is forced unification.
So is ignoring trade-offs.
So is treating noise as signal.
So is misjudging physiologic reserve.
Orientation defines what kind of reasoning is appropriate before that reasoning begins.
Thinking
Thinking assigns and revises cognitive weight within the terrain Orientation has defined.
Thinking is not diagnosis.
Thinking is disciplined judgment under uncertainty.
Thinking is where you decide:
- which possibilities deserve the most attention right now
- which ones carry the greatest potential harm if missed
- which ones can safely wait
- which ones may be contextual noise
- how much uncertainty you can tolerate at this moment
Thinking is not just listing causes.
Thinking is not just naming the most likely diagnosis.
Thinking is not just running an algorithm.
Thinking is deciding how much each possibility should matter in this specific situation.
In Consult Practice, Thinking is not only Bayesian ranking.
It is priority-setting under uncertainty and asymmetric risk.
You are not only asking:
“What is most likely?”
You are also asking:
“What matters most if I am wrong?”
Thinking preserves cognitive flexibility.
It allows vigilance without alarm, restraint without passivity, and revision without defensiveness.
Execution
Execution makes judgment visible.
Execution is not simply what you do.
It is how your internal judgment becomes operative at the bedside.
Execution is the translation of stance into:
- protection
- prioritization
- communication
- timing
- and revision
Execution is where uncertainty is made safe for patients and teams.
Execution is not the checklist.
Execution is not the order set.
Execution is not simply “doing things.”
Execution is how consultant judgment becomes shared, timed, and protective in real time.
Without Execution, judgment remains private.
Private judgment does not protect patients.
Execution is downstream of Thinking in logic, but simultaneous with Thinking in time.
Consultants often execute while still thinking, and think while already executing:
“Let’s do this for now, but I’m not convinced yet.”
That is Thinking and Execution running in parallel.
Execution is judgment-in-motion.
Situational Awareness and Why Orientation Comes First
Orientation is best understood as situational awareness, a concept widely used in aviation, emergency response, and military operations.
Situational awareness answers three questions:
- What is happening?
- What could happen next?
- How much uncertainty is tolerable before action becomes unsafe?
In medicine, failures often occur not because clinicians lack knowledge, but because they commit too early—to a diagnosis, to reassurance, or to escalation—before situational awareness is established.
Orientation exists to prevent that error by defining the terrain before analytical reasoning and action proceed.
Orientation tells you what kind of clinical world you are standing in.
Only then can Thinking and Execution proceed safely.
How Orientation, Thinking, and Execution Fit Together
In Consult Practice, judgment unfolds across three linked layers:
Orientation
What kind of problem is this?
- Am I in a competing-harms terrain?
- Is this a fast-moving, dangerous process?
- Is this likely signal versus contextual noise?
- Is premature closure dangerous here?
Orientation selects the governing logic.
It chooses the rules of reasoning.
Thinking
Within those rules, what should I weight most heavily right now?
Thinking is where you:
- rank hypotheses
- assign probabilities (even if implicitly)
- decide what you are most worried about
- decide what you are willing to tolerate
- decide what uncertainty you can live with for now
This is where analytic reasoning lives.
This is also where intuition can live—but only within the terrain Orientation has defined.
Thinking is not free-form.
It is constrained by the kind of problem you have already identified.
Execution
Given what I think matters most, what do I actually do and say?
Execution is where you:
- order tests
- start or stop treatments
- communicate urgency
- explain uncertainty
- coordinate with teams
- and protect the patient from harm
Execution makes your Thinking visible.
Different Terrains Demand Different Kinds of Thinking
A defining feature of Consult Practice is that each disease module names the dominant cognitive force at play, rather than applying a single reasoning style to every situation.
Consult Practice organizes judgment by cognitive demand, not just by diagnosis.
| Clinical Domain | Dominant Cognitive Force | Governing Question |
|---|---|---|
| Neutropenia | Reserve-threat reasoning | Is host defense insufficient right now? |
| Anticoagulation + bleeding | Competing-harms reasoning | Which danger dominates if I act or don’t act? |
| Leukocytosis | Signal-discrimination reasoning | Is this a dangerous signal or contextual noise? |
| Severe anemia | Threshold / tempo reasoning | Has physiologic reserve crossed a dangerous limit? |
| Suspected hemolysis | Pattern-discrimination reasoning | Does this pattern mean what it appears to mean? |
| Thrombocytopenia | Plausibility-weighting reasoning | Which explanations deserve attention given base rates, context, and trajectory? |
The same laboratory value can require vigilance, restraint, or immediate protection depending on the terrain, the trajectory, and the dominant reasoning problem.
Recognizing which kind of thinking the moment demands is the skill being taught.
Two Familiar Metaphors for Expert Judgment
Consult Practice does not teach answers.
It teaches how experts decide what kind of situation they are in before answering.
| Consult Practice | Detective | Fire Response |
|---|---|---|
| Orientation | Arrives at the scene, establishes situational awareness | Alarm assessment: smoke, fire, malfunction, or false trigger |
| Thinking | Weighs competing hypotheses and leads | Command judgment: contain, ventilate, evacuate, monitor |
| Execution | Interviews, searches, team communication | Deploy hoses, ventilate, evacuate, or observe |
A detective who interrogates before understanding the scene creates false narratives.
A fire crew that charges in without assessing the alarm risks catastrophe.
Likewise, consultants who act before clarifying terrain or assigning cognitive weight confuse speed with judgment.
Why Consult Practice Is Different
Most educational resources organize knowledge by diagnosis.
Consult Practice organizes judgment by cognitive demand.
Reference texts assume Orientation has already occurred.
They assume the problem space is already defined.
Consult Practice makes that upstream cognitive work explicit.
It shows:
- how experts define the terrain
- how they assign and revise cognitive weight
- how they make judgment visible through safe execution
This is the invisible architecture of expert consult medicine.
How to Use Consult Practice
Each disease-specific hub brings together three coordinated pieces:
Orientation — to establish situational awareness and define the terrain
Thinking — to show how experts assign and revise cognitive weight under uncertainty
Execution — to make judgment visible through action and communication
These pieces are not meant to be read linearly at the bedside.
They are designed to be consulted, revisited, and compared across conditions and clinical contexts.
They do not replace reference texts.
They explain the cognitive work that reference texts assume has already occurred.