How expert consultants define terrain, assign weight, and make judgment visible when two blood counts fall together and premature unification can be dangerous.
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Two Abnormalities, One Judgment Problem
Anemia with thrombocytopenia is not just “two low counts.”
It is a commitment-timing problem.
When hemoglobin and platelets fall together, clinicians are naturally drawn toward coherence. A single explanation feels elegant. A shared diagnosis feels efficient. A unifying story feels satisfying.
Sometimes that instinct is lifesaving.
Sometimes it is misleading.
And sometimes the danger has little to do with whether the abnormalities share a cause at all.
The same laboratory pattern can live in very different clinical worlds:
- a catastrophic unifying process requiring urgent action
- two separate problems that happen to overlap in time
- a dominant issue with a second abnormality acting as noise
- evolving physiology where trajectory matters more than mechanism
- a stable patient where restraint is safer than escalation
In each case, the numbers may look similar.
The danger is not.
This is why anemia with thrombocytopenia is not primarily a diagnostic problem.
It is a judgment problem.
Expert consultation is not about choosing one story quickly.
It is about deciding when a story deserves commitment.
Consult Practice makes that expert judgment visible.
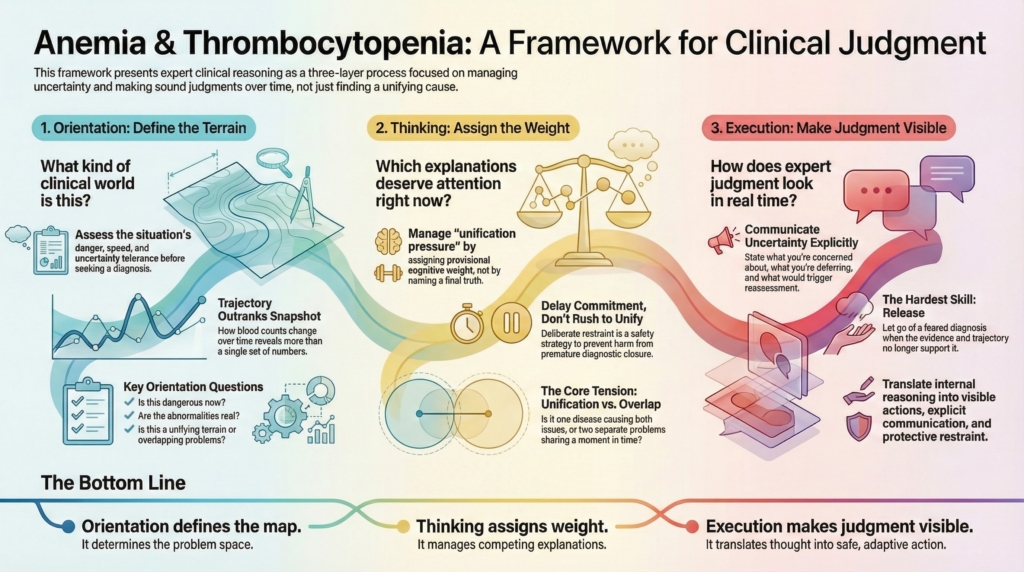
The Three-Layer Framework: Orientation, Thinking, Execution
This series approaches anemia with thrombocytopenia through three distinct cognitive layers:
- Orientation — defining the terrain
- Thinking — assigning weight within that terrain
- Execution — making judgment visible through action and communication
Each layer has a different job.
Confusing them is one of the most common sources of clinical error.
Together, they protect against premature commitment, forced coherence, and delayed release when biology evolves.
Orientation Defines the Map
Orientation answers a simple but powerful question:
What kind of clinical world am I in right now?
Orientation is not diagnosis.
It is terrain definition.
In anemia with thrombocytopenia, Orientation clarifies:
- how dangerous this situation could be right now
- how fast it may evolve
- how much uncertainty can be safely tolerated
- whether a systemic or destabilizing terrain is plausible
- whether overlap versus unification is even a meaningful question yet
Orientation helps distinguish between worlds such as:
- narrow, high-risk terrain (e.g., microangiopathic or thrombotic patterns)
- bleeding-dominant terrain
- consumptive or inflammatory systemic terrain
- marrow-dominant terrain
- overlapping-problem terrain
- broader, stable physiologic terrain
These are not causes.
They are problem spaces.
Orientation often begins at the time of the page.
But it is not a one-time act.
Whenever trajectory, stability, or clinical context changes, Orientation must be re-invoked.
Orientation answers:
What kind of situation is this?
Thinking Assigns Weight Within the Defined World
Once the terrain is defined, Thinking takes over.
Thinking answers a different question:
Within this world, which explanations deserve the most cognitive weight right now?
In anemia with thrombocytopenia, Thinking is governed by a unique problem:
unification pressure.
Two abnormalities invite coherence.
But coherence can be dangerous.
Thinking focuses on:
- whether the abnormalities plausibly share a cause
- whether they more likely represent overlapping problems
- how trajectory strengthens or erodes unifying explanations
- how much weight any one frame deserves at this moment
- how long a hypothesis should be allowed to shape vigilance
- when restraint is safer than consolidation
Thinking is where expert consultants:
- delay premature commitment
- manage Ockham and Hickam as a timing problem
- assign provisional weight rather than naming truth
- hold competing explanations safely
- practice release when biology no longer supports earlier concern
Thinking answers:
Which explanations deserve attention right now, and what would change that?
Execution Makes Judgment Visible
Execution is where judgment becomes real to others.
Execution answers:
What must be clarified, protected, communicated, deferred, and revisited — right now?
In anemia with thrombocytopenia, Execution is shaped by:
- whether a dangerous unifying process must be actively protected against
- whether overlap requires managing two risks simultaneously
- whether restraint is safer than escalation
- how urgency and vigilance are signaled to the team
- how uncertainty is transmitted explicitly
- how recalibration is made visible over time
Execution is not running a checklist.
It is translating judgment into safe clinical behavior as biology evolves.
Execution includes:
- first safety passes
- protective escalation
- visible restraint
- explicit communication of uncertainty
- defined reassessment triggers
- transparent recalibration
This is why Execution is best described as:
Judgment made visible.
Execution answers:
How does expert judgment look in real clinical time?
Why This Framework Matters
Many errors in anemia with thrombocytopenia do not arise from lack of knowledge.
They arise from:
- forcing unification because it feels elegant
- anchoring on a feared diagnosis too early
- assuming overlap because unification feels uncomfortable
- allowing early labels to drive momentum
- failing to release concern when trajectory no longer supports it
- confusing explanation with danger management
This framework protects against category failure:
- treating dual abnormalities like a single-cause puzzle
- treating evolving physiology like a static snapshot
- treating uncertainty as something to eliminate rather than manage
By separating Orientation, Thinking, and Execution, the consultant:
- defines the correct terrain
- assigns weight deliberately
- and makes judgment visible and revisable
This is how expert consultants protect patients when two blood counts fall together and the stakes are real.
How to Use This Series
This overview is the conceptual front door.
The three companion essays go deeper:
- Orientation — for defining the problem space
- Thinking — for managing unification pressure, weighting, and commitment timing
- Execution — for visible action, communication, and recalibration over time
They are designed to be used together.
Not as algorithms.
Not as diagnostic manuals.
But as a guide to how expert consultants think, act, and recalibrate when anemia and thrombocytopenia coexist.
Bottom Line
Anemia with thrombocytopenia is not a diagnosis.
It is a commitment-timing signal.
Expert care depends on:
- defining what kind of world the patient is in
- assigning cognitive weight to shared versus overlapping explanations deliberately
- and making judgment visible through safe, adaptive execution
Orientation defines the map.
Thinking assigns weight.
Execution makes judgment visible.
That is how hematologists reason when two blood counts fall together and the stakes are real.