How expert consultants use a five-module method to manage unification pressure, evolving danger, and commitment timing when two blood counts fall together
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why a Five-Module System
Anemia with thrombocytopenia is not a single problem.
It is a pattern that creates unification pressure.
Two abnormalities invite coherence.
A single explanation feels elegant.
A shared diagnosis feels efficient.
But in real consult medicine, the central risk is not missing a rare diagnosis.
The central risk is misclassifying the terrain and committing too early or releasing too late.
This is why Consult Practice uses a five-module system.
Each module does a different kind of cognitive work.
Together, they form a method for managing uncertainty over time, not a list of causes.
The modules are designed to:
- constrain probability without premature diagnosis
- define what should change your posture
- preserve vigilance for rare catastrophic terrain
- train category discipline
- and support rapid bedside judgment under pressure
They are meant to be used together.
Not as a checklist.
Not as a curriculum.
But as a reusable consult discipline.
The Five Modules and What Each One Does
Module 1 — Most Likely in This Context
Early weighting by terrain and tempo
What it does:
Constrains probability without diagnosis.
This module answers:
Given this setting, trajectory, and severity, what deserves the most attention right now?
In anemia with thrombocytopenia, Module 1 helps you:
- weight risk by location (ED, ICU, ward, L&D, cirrhosis unit, etc.)
- interpret timing (parallel vs discordant declines)
- understand how severity narrows the terrain
- set early urgency without declaring a cause
This is where you learn:
What should I be most worried about first, in this context?
Module 1 shapes initial vigilance, not conclusions.
Module 2 — What Would Change the Posture
Trajectory- and trigger-based reassessment
What it does:
Defines what new data should escalate concern, narrow the signal, or justify safe release.
This module answers:
What would make me think differently in six hours, tomorrow, or after new labs?
In anemia with thrombocytopenia, Module 2 teaches:
- which signals push toward a shared high-risk terrain
- which signals favor overlapping, non-unifying physiology
- when severity alone should force posture change
- how trajectory reshapes meaning over time
This module makes recalibration explicit.
It trains the consultant to ask:
Has the terrain changed, and should my posture change with it?
Module 3 — Disease-Specific Applied Danger Frame
When this pattern is dangerous in itself
What it does:
Preserves vigilance for rare but catastrophic terrain unique to specific diseases.
This module answers:
When does this pattern stop being just a signal and become a direct threat?
For anemia with thrombocytopenia, this includes terrains such as:
- TTP / MAHA physiology
- acute leukemia / marrow failure
- severe systemic consumptive states
- hemolytic infections such as babesiosis
Module 3 is not a differential.
It is a danger frame.
It teaches:
In which diseases does delay itself become dangerous?
This module protects against under-recognition of catastrophic terrain.
Module 4 — Boundary Drill (Practice & Reflection)
Orientation vs Thinking vs Execution
What it does:
Trains category discipline and prevents lens drift.
This module answers:
Am I defining terrain, assigning stance, or directing visible action?
Through cases, Module 4 teaches:
- how location, timing, and severity shape posture
- how experts avoid premature commitment
- how misclassification of terrain leads to common consult errors
- how judgment is revised safely over time
This is where trainees learn:
Not just what to think,
but how expert consultants think and recalibrate.
This module makes the method teachable.
Module 5 — Quick-Access Card
Compressed bedside cognitive map
What it does:
Provides a rapid posture reminder under pressure.
This module answers:
What stance should I adopt right now?
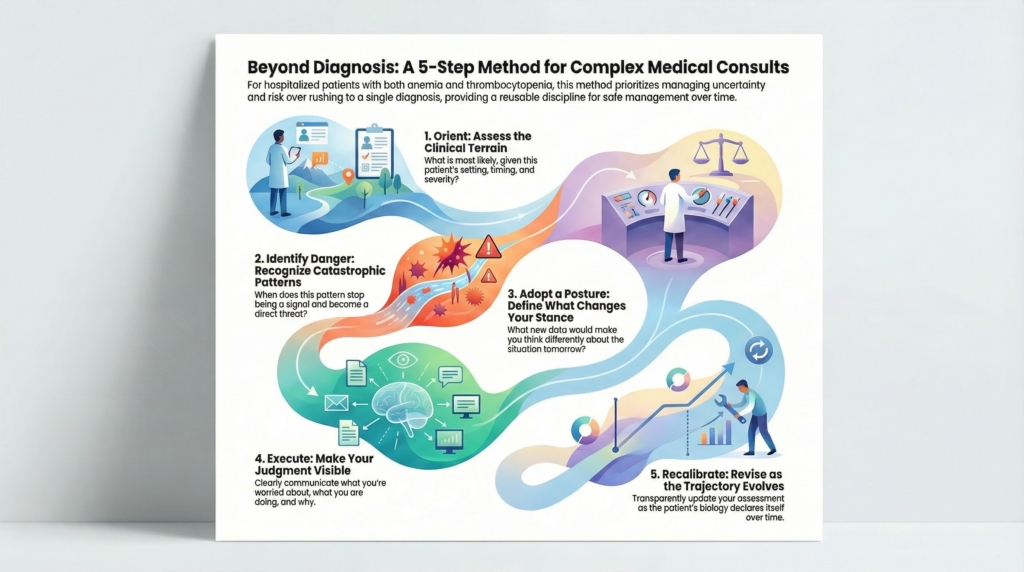
Through O → D → T → E → R cards, Module 5 supports:
- fast orientation
- danger recognition
- provisional framing
- visible execution
- and recalibration
This is not a shortcut for thinking.
It is a memory aid for posture.
It is where Consult Practice becomes usable at 2 a.m.
Why This Architecture Matters
Many consult errors in anemia with thrombocytopenia do not arise from lack of knowledge.
They arise from:
- forcing unification too early
- anchoring on feared diagnoses
- treating dual abnormalities as a single-cause puzzle
- failing to revise posture as trajectory evolves
- confusing explanation with danger management
The five-module system prevents category failure by separating:
- early weighting from diagnosis
- trajectory from static snapshots
- disease danger from pattern recognition
- teaching from doing
- and compression from reasoning
It turns a complex consult pattern into a repeatable cognitive method.
How to Use This Series
This overview is the architectural front door.
The modules are designed to be used together:
- Module 1 sets early attention
- Module 2 defines what changes posture
- Module 3 preserves vigilance for rare catastrophe
- Module 4 trains judgment and lens discipline
- Module 5 supports real-time bedside use
They are not linear.
They are recursive.
They reflect how real consult judgment evolves as biology declares itself.
Bottom Line
Anemia with thrombocytopenia is not a diagnosis.
It is a pattern that creates unification pressure, evolving danger, and commitment timing.
This five-module system teaches consultants how to:
- constrain probability safely
- recognize when posture should change
- preserve vigilance for catastrophic terrain
- practice disciplined judgment
- and support real-time decision-making
Not as algorithms.
Not as cause lists.
But as a method for expert consult medicine.