Defining the Clinical Terrain
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
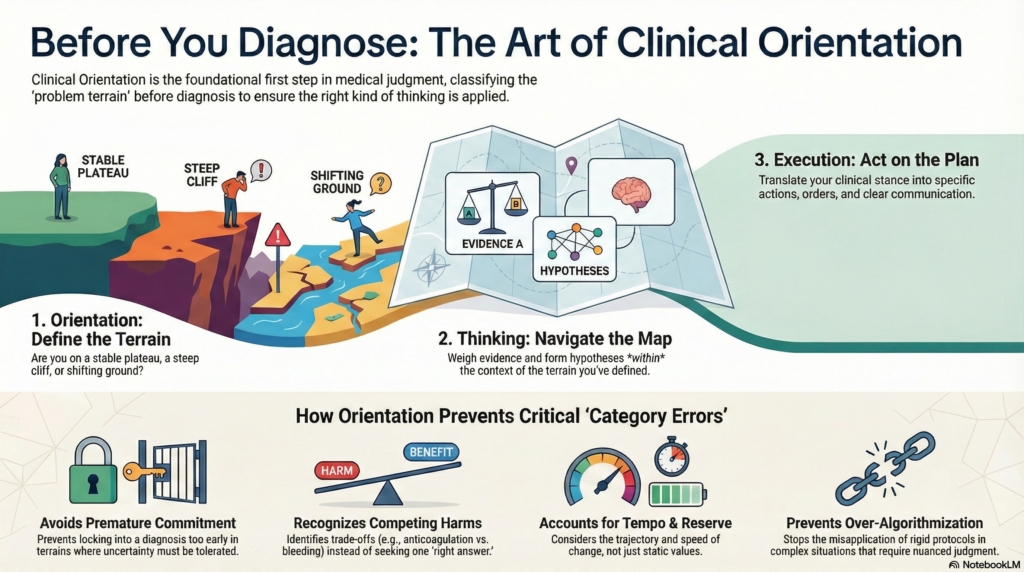
Before deciding what a patient has, consultants decide what kind of situation they are in.
This is the work of Orientation.
Orientation is not diagnosis.
It is not a list of tests.
It is not a management plan.
Orientation is a form of thinking, but it is a different kind of thinking than diagnosis, probability-weighting, or decision-making. It is the disciplined act of locating yourself in the problem space before you decide how to reason or act.
Orientation answers a different set of questions:
- What kind of situation is this?
- What kinds of danger are plausible right now?
- How urgent is this moment?
- How much uncertainty can safely be tolerated?
- How fast might this picture change?
In other words, Orientation defines the terrain.
It tells you whether you are standing on:
- a stable plateau,
- a steep cliff,
- shifting ground,
- or a narrow bridge where small errors carry large consequences.
Only after you know the terrain does it make sense to decide:
- how to think (what to weight, what to hold in suspension), and
- how to act (what to protect, escalate, defer, or communicate).
Orientation sets the map.
Thinking and Execution happen inside that map.
Without a defined terrain, even expert reasoning has no reference frame.
Orientation is not situational awareness
Orientation includes situational awareness, but it is not identical to it.
Situational awareness is about:
- noticing what is happening,
- tracking what has changed, and
- anticipating what might happen next.
Orientation goes further.
Orientation takes situational awareness and uses it to define the rules of the game:
- Is this a problem where delay is dangerous?
- Is this a problem where restraint is safer than action?
- Is this a problem where being wrong carries asymmetric harm?
- Is this a problem where premature closure is the main risk?
Situational awareness tells you what you see.
Orientation tells you what kind of clinical world you are in.
This is why Orientation is architectural.
It does not compete with Thinking and Execution.
It contains them.
Why good thinking fails without Orientation
When Orientation is skipped, consultants often reason well — about the wrong problem.
A falling hemoglobin is treated as iron deficiency before asking whether the patient is actively bleeding.
Thrombocytopenia is worked up as ITP before asking whether the patient is septic.
A low platelet count triggers transfusion before asking whether the trajectory suggests consumptive coagulopathy.
These are not failures of knowledge.
They are failures of Orientation.
They represent category errors: applying the wrong kind of reasoning to the wrong kind of terrain.
Orientation exists to prevent category error — applying diagnostic, algorithmic, or unifying logic to problems that require a different governing cognitive force.
Orientation does not resolve uncertainty.
It classifies what kind of uncertainty you are in.
Orientation is classification, not computation
This is a critical distinction.
Orientation does not analytically sort out trade-offs.
Orientation recognizes that you are in a trade-off terrain at all.
Orientation does not decide whether a lab value is signal or noise.
Orientation recognizes that this is a signal-discrimination terrain.
Orientation does not weigh competing hypotheses.
Orientation recognizes that multiple hypotheses must remain live.
Orientation is not where you do the math.
Orientation is where you choose which math problem you are solving.
More precisely:
- Orientation = pre-analytic structural recognition
- Thinking = analytic weighting and revision within that structure
- Execution = translation of stance into action and communication
Orientation is the act of recognizing what kind of reasoning will be required, before that reasoning is performed.
The terrains Orientation protects against
Orientation guards against several classes of error. Each reflects a different kind of terrain that, if unrecognized, leads to predictable mistakes.
1. Premature commitment
Locking into a diagnosis
Closing the hypothesis space too early
Treating uncertainty as if it is already resolved
This is common, but not universal. Some terrains punish premature closure more than others. Orientation determines whether this is one of them.
2. Forced unification
Trying to explain everything with one story when the terrain is actually mixed.
Examples:
- Assuming two abnormalities must represent one disease
- Forcing a single mechanism when physiology is bifurcated
- Treating overlapping processes as if one must be wrong
Orientation allows plural terrains to coexist.
3. Failure to recognize trade-offs
Not seeing that the terrain is governed by competing harms.
Examples:
- Anticoagulation vs bleeding
- Infection vs marrow suppression
- Oxygen delivery vs volume overload
Without Orientation, clinicians act as if there is a “right answer,” when the terrain is actually optimization under conflict.
4. Misclassification of signal vs noise
Treating contextual physiology as pathology, or pathology as context.
Examples:
- Stress leukocytosis
- Reactive thrombocytopenia
- Transient lab abnormalities
Orientation defines whether this is a signal-discrimination terrain at all.
5. Failure to recognize tempo and reserve
Ignoring trajectory and physiologic buffer.
Examples:
- Stable severe anemia vs rapidly falling moderate anemia
- Stable neutropenia vs crashing neutropenia with sepsis
Orientation defines whether tempo and reserve govern safety.
6. Over-algorithmization
Applying the wrong reasoning style to the wrong terrain.
Examples:
- Using diagnostic matching in a competing-harms terrain
- Using protocols when stance should dominate
- Using unification when plural processes are likely
Orientation is what selects the governing cognitive force.
Structural summary: what Orientation actually does
Orientation does not solve these problems.
It makes certain mistakes structurally unavailable by classifying the terrain first.
Once the terrain is classified:
- Some reasoning styles become mandatory
- Others become unsafe
- Some questions become illegitimate
This is how Orientation protects judgment.
Terrain, governing logic, and category error
Here is a formal way to make this visible:
| Terrain Feature | What Orientation Recognizes | What Thinking Then Must Do | Category Error Orientation Prevents |
|---|---|---|---|
| Competing harms | This is a trade-off terrain | Optimize between harms | Treating as single “right answer” |
| Signal vs noise | This is a discrimination terrain | Separate context from pathology | Treating noise as disease |
| Plural processes | This terrain allows multiple causes | Keep hypotheses live | Forced unification |
| Tempo & reserve | Trajectory governs danger | Weight speed and buffer | Static threshold thinking |
| High uncertainty | Premature closure is dangerous | Delay commitment | Early diagnostic lock-in |
| Judgment terrain | Algorithms are unsafe | Use stance-based reasoning | Protocol dominance |
Orientation does not compute these trade-offs.
It recognizes which logic governs.
That recognition changes everything downstream.
Orientation as architectural frame
Orientation exists to correctly define the problem terrain so that the right kind of thinking and execution become possible.
More precisely:
Orientation exists to prevent category error — applying the wrong kind of reasoning to the wrong kind of problem.
Premature commitment is one form of category error.
So are forced unification, ignoring trade-offs, treating contextual noise as diagnostic signal, misjudging physiologic reserve, or applying algorithmic logic to problems that require judgment under uncertainty.
Orientation does not resolve these problems.
It classifies the terrain so that the appropriate reasoning posture becomes available.
This is why Orientation is not optional.
It is not preliminary.
It is structural.
It is the frame that gives Thinking and Execution their meaning.
Orientation is not a one-time event
Orientation is not something that happens only when the pager goes off.
It is not confined to the beginning of a consult.
Orientation is atemporal.
It can — and often must — be revisited whenever the terrain changes:
- when new data arrives,
- when a trajectory accelerates or stabilizes,
- when a patient decompensates,
- when an assumption is challenged,
- or when the balance of risk shifts.
A consult may begin in one terrain and evolve into another.
Expert consultants re-orient.
They do not just update probabilities.
They reclassify what kind of problem they are in.
This is not changing one’s mind about a diagnosis.
It is changing one’s mind about the rules of the game.
Architectural Note: Orientation and Thinking
(Sidebar / callout box)
Orientation involves thinking.
But it is not the same kind of thinking as what the Thinking lens is responsible for.
Consult Practice does not divide judgment into “thinking vs acting.”
It divides judgment by functional role in the architecture of clinical judgment.
More precisely:
- Orientation = terrain classification
(What class of problem is this?) - Thinking = weighting within terrain
(Within this class, what matters most right now?) - Execution = translation into action and communication
(What must be done and said so others act safely?)
These are three different computational problems.
If Orientation is folded into Thinking, a critical architectural boundary is lost. Clinicians begin weighting hypotheses before they have classified what kind of problem they are in. That is exactly the failure mode this framework is designed to prevent.
Orientation is meta-cognitive.
It selects which reasoning mode is appropriate.
Thinking is object-level.
It operates within the selected mode.
This is the difference between:
- choosing the right map vs navigating the road,
- choosing the right statistical model vs running the regression,
- choosing the right imaging modality vs interpreting the scan.
Both require thinking.
They are not the same function.
Orientation is therefore a form of thinking — but it is not the same cognitive operation as Thinking in Consult Practice. Orientation classifies the type of problem. Thinking assigns weight within that type.