How to use focused cognitive tools to support safe judgment when platelet counts are low and the stakes are real.
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
What these modules are
These modules are not Orientation, Thinking, or Execution essays.
They are practical cognitive tools designed to support consultants within those lenses — at the bedside, during rounds, and as the clinical picture evolves.
They exist to make expert posture easier to access in real time.
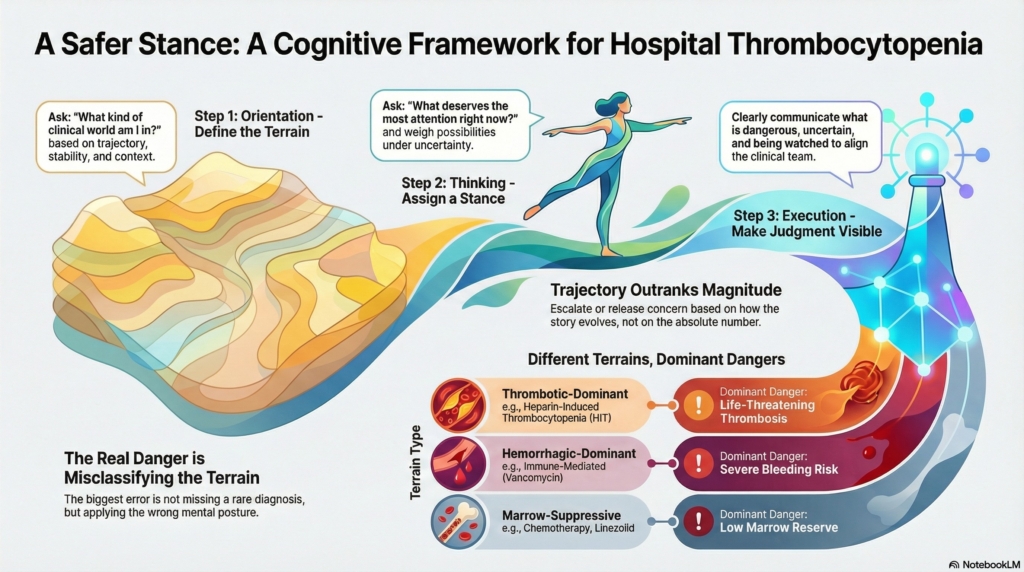
If Orientation defines the map,
and Thinking defines stance,
and Execution makes judgment visible,
then these modules are working instruments — tools you can pick up to:
- test whether your posture still fits the terrain
- recalibrate concern as data evolve
- practice separating terrain, stance, and action
- and communicate uncertainty safely
They are designed for use in motion, not for linear reading.
Why modules matter in thrombocytopenia
Thrombocytopenia is common in hospitalized patients.
Most cases are related to infection, medications, or systemic illness.
A smaller subset represents marrow failure, thrombotic microangiopathy, or competing-harm physiology.
The danger is not missing a rare diagnosis.
The danger is misclassifying the terrain and applying the wrong posture:
- treating a tempo-driven problem as a slow diagnostic puzzle
- treating a competing-harms situation as a single-threat problem
- or reassuring prematurely based on a single number
These modules exist to help you recognize, weight, and communicate risk before biology has fully declared itself.
They are built to reduce category failure.
How these modules fit with Orientation, Thinking, and Execution
Each module deliberately touches all three lenses — but with a specific function.
They are not replacements for the core essays.
They are extensions that make the lenses usable in practice.
Across modules:
- Orientation is reinforced by terrain detection, trajectory awareness, and context recognition
- Thinking is reinforced by weight assignment, posture shifts, and vigilance logic
- Execution is reinforced by communication patterns, escalation thresholds, and visible restraint
The goal is not to add content.
The goal is to make expert judgment easier to deploy under uncertainty.
How to use these modules
These modules are meant to be used:
- at the time of the page
- during rounds
- when new labs arrive
- when posture feels uncertain
- or when teaching trainees how consultants actually think
They are especially useful when:
- the platelet count is changing
- the team is anxious
- the number is symbolic
- or the clinical story is incomplete
They can be used individually or together.
They are designed to be revisited.
The thrombocytopenia modules in this set
This thrombocytopenia series includes five focused tools:
Quick-Access Card
A rapid bedside cognitive map to align Orientation, Thinking, Execution, and recalibration when platelet counts are low.
Use when you need a compressed posture reminder.
Most Likely in This Context
A context-driven tool that shows how care setting and terrain shift what thrombocytopenia most plausibly represents.
Use when the number is the same, but the clinical world is different.
What Would Change the Posture
A trajectory-based module that identifies what new data should escalate or release concern.
Use when deciding whether vigilance should increase, decrease, or remain unchanged.
Medication-Associated Thrombocytopenia
A focused terrain module that helps distinguish medication-related decline from consumptive, marrow, or thrombotic processes — including immune-mediated thrombocytopenia and heparin-induced thrombocytopenia.
Use when tempo, exposure, and recovery patterns suggest a drug-related terrain.
Boundary Drill: Orientation, Thinking, or Execution
A teaching and reflection tool to practice separating:
- terrain definition
- stance assignment
- and visible action
Use to reduce category errors and improve consult reasoning clarity.
How these modules differ from reference resources
These modules are not protocols.
They do not replace:
- institutional pathways
- transfusion thresholds
- diagnostic algorithms
- or guideline-driven workups
They operate upstream of those tools.
They help ensure that the right resources are applied to the right terrain.
They are designed to support judgment before certainty.
A note on uncertainty and recalibration
A central principle across all modules is this:
Release by non-progression is as important as escalation.
Expert consult practice is not defined by how fast you escalate.
It is defined by how precisely you:
- escalate when danger is plausible
- hold vigilance when uncertainty remains
- and release concern when biology fails to reinforce feared trajectories
These modules are built to support that discipline.
Bottom line
Thrombocytopenia in the hospital is not a diagnosis.
It is a signal.
These modules are designed to help you:
- recognize what kind of world you are in
- decide what deserves attention
- make judgment visible
- and revise posture as the story evolves
They are tools for thinking in motion.
They exist to make consult judgment safer, clearer, and more teachable.