When the CBC Doesn’t Make Sense
When the CBC Doesn’t Make Sense
Cold agglutinin disease masquerading as laboratory inconsistency
By William C. Aird, MD
Case Presentation
A 66-year-old woman with beta-thalassemia trait and chronic malnutrition was admitted after being found collapsed outside her apartment.
On arrival she was:
- hypoglycemic (glucose 25 mg/dL)
- hypothermic (rectal temperature 84°F)
Her hospitalization was complicated by several findings, including:
- newly diagnosed systolic heart failure
- pericardial effusion
- possible chronic liver disease
- cavitary lung lesion
Hematology was consulted for anemia and a positive direct antiglobulin test.
Laboratory Findings
On admission:
| Test | Result |
|---|---|
| Hemoglobin | 6.6 g/dL |
| LDH | 699 U/L |
| Indirect bilirubin | elevated |
| Haptoglobin | <10 mg/dL |
A direct antiglobulin test (DAT) was positive.
A cold agglutinin screen was also positive.
In the setting of profound hypothermia (84°F), cold-reactive antibodies may promote red cell agglutination and hemolysis centrally rather than only in the periphery. Rewarming therefore becomes both supportive care and a physiologic intervention that can reduce cold-mediated hemolysis.
A Curious Pattern
Repeated CBC measurements showed two different patterns:
| Situation | MCV | RDW |
|---|---|---|
| Unwarmed samples | high MCV | very high RDW |
| Warmed samples | low MCV | lower RDW |
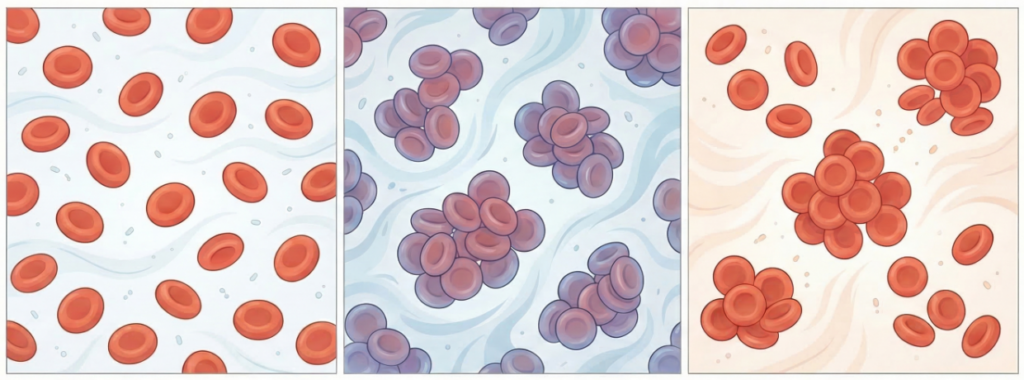
Peripheral smear showed diffuse red cell agglutination.
When CBC values are internally inconsistent or contradict the patient’s known physiology, clinicians should consider a pre-analytic artifact rather than assuming the numbers are correct. In this setting, the smear and the warmed sample become essential tools for recovering the true hematologic picture.
What is the most likely explanation for the changing MCV values?
Explanation
Cold agglutinins cause red cells to clump together when blood cools.
Automated analyzers may interpret RBC clumps as single large cells, leading to:
- falsely elevated MCV
- falsely elevated RDW
- inconsistent CBC results
When samples are warmed before analysis, the clumps disperse and the true RBC indices are revealed.
This case is especially instructive because the artifact does not merely distort the CBC, it reverses the apparent phenotype. The unwarmed sample suggests macrocytosis, whereas the warmed sample reveals the patient’s underlying microcytosis from beta-thalassemia trait.
Additional Context
Beta-thalassemia trait normally produces:
- mild anemia
- low MCV
When her blood samples were warmed, the CBC showed:
- microcytosis
- indices consistent with her baseline thalassemia trait
This illustrates a broader principle: when two processes affect the same parameter in opposite directions, one may temporarily mask or invert the other. Here, cold agglutinin–related agglutination concealed the patient’s expected microcytosis.
Which of the following laboratory findings is most characteristic of cold agglutinin disease?
Explanation
Cold agglutinins are typically IgM antibodies that activate complement.
As a result:
- the DAT is positive for C3
- the DAT is usually negative for IgG
This pattern distinguishes CAD from warm autoimmune hemolytic anemia.
Differential Diagnosis of Cold-Related Antibodies
Three major antibody types can be associated with cold exposure:
| Disorder | Antibody | Key feature |
|---|---|---|
| Cold agglutinin disease | IgM | RBC agglutination |
| Paroxysmal cold hemoglobinuria | Donath–Landsteiner antibody | intravascular hemolysis |
| Cryoglobulinemia | immune complexes | vasculitis |
In this patient, the presence of overt RBC agglutination on smear strongly favored cold agglutinin disease over paroxysmal cold hemoglobinuria or cryoglobulinemia.
Which of the following is an important supportive measure for patients with cold agglutinin disease?
Explanation
Cold exposure promotes:
- antibody binding
- complement activation
- hemolysis
Patients with CAD should therefore:
- maintain euthermia
- avoid cold exposure
- receive warmed blood products when transfusions are needed
In this case, rewarming was particularly important because the patient was profoundly hypothermic. At such low core temperatures, cold agglutinin activity is no longer confined to acral circulation and may contribute directly to systemic hemolysis.
Teaching Points
- Cold agglutinin disease can produce dramatic laboratory artifacts.
Spurious macrocytosis and marked RDW elevation may occur when red cells agglutinate in cooled samples. - When the CBC does not fit the patient’s known physiology, the peripheral smear becomes essential.
Reviewing the smear and repeating the CBC on a warmed sample can reveal the patient’s true red cell indices. - Cold agglutinin–related artifact may mask an underlying hematologic condition.
In this patient, warming the sample revealed the expected microcytosis of beta-thalassemia trait. - Rewarming is not merely supportive in severe hypothermia.
By reducing cold-induced agglutination, restoration of normal body temperature may directly lessen hemolysis.
Why This Case Matters
Many clinicians first encounter cold agglutinin disease not through symptoms, but through bizarre laboratory results.
This case highlights a particularly important pattern:
- RBC agglutination on smear
- inconsistent CBC indices
- normalization of indices with warming
It also shows that cold agglutinin disease may appear in medically complex patients with multiple competing explanations for anemia. Recognizing when the CBC is being distorted by cold-induced agglutination allows clinicians to recover the patient’s true hematologic baseline and avoid diagnostic confusion.