When the Blood Type Suddenly Changes
When the Blood Type Suddenly Changes
Cold agglutinins interfering with blood bank testing
By William C. Aird, MD
Case Presentation
A 68-year-old man with:
- end-stage renal disease on hemodialysis
- diabetes mellitus
- hepatitis C
- recent MRSA bacteremia
was admitted with severe anemia.
His hemoglobin had fallen to the 5–7 g/dL range, and transfusion was planned.
During compatibility testing, the blood bank reported a striking finding:
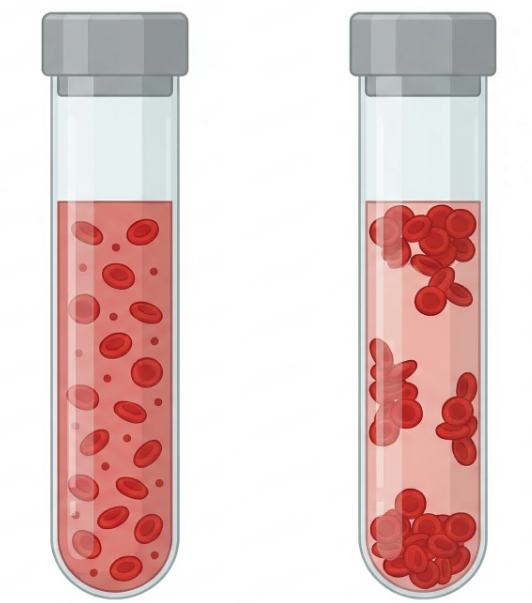
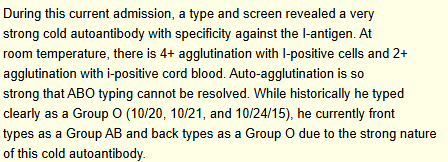
“A very strong cold autoantibody with specificity against the I antigen.
Auto-agglutination is so strong that ABO typing cannot be resolved.”
Historically, the patient had consistently typed as blood group O.
During this admission, however:
| Test | Result |
|---|---|
| Forward typing | AB |
| Reverse typing | O |
Blood bank report:
ABO typing discrepancies are not merely a laboratory curiosity. In patients who require urgent transfusion, failure to recognize cold agglutinin interference can delay the safe selection of compatible blood products.
This patient’s recent MRSA bacteremia reflects severe systemic illness, which can exacerbate hemolysis through complement activation and physiologic stress. However, the identification of a strong anti-I cold autoantibody in a 68-year-old patient without evidence of Mycoplasma infection raises the possibility of underlying cold agglutinin disease (CAD) rather than transient infection-associated cold agglutinin syndrome. In this setting, the MRSA infection may represent either a trigger that brought the hemolysis to clinical attention or simply an incidental comorbidity.