Venous Thrombosis in Lower Extremities – Treatment Overview
Prev
1 / 2
Next
Prev
1 / 2
Next
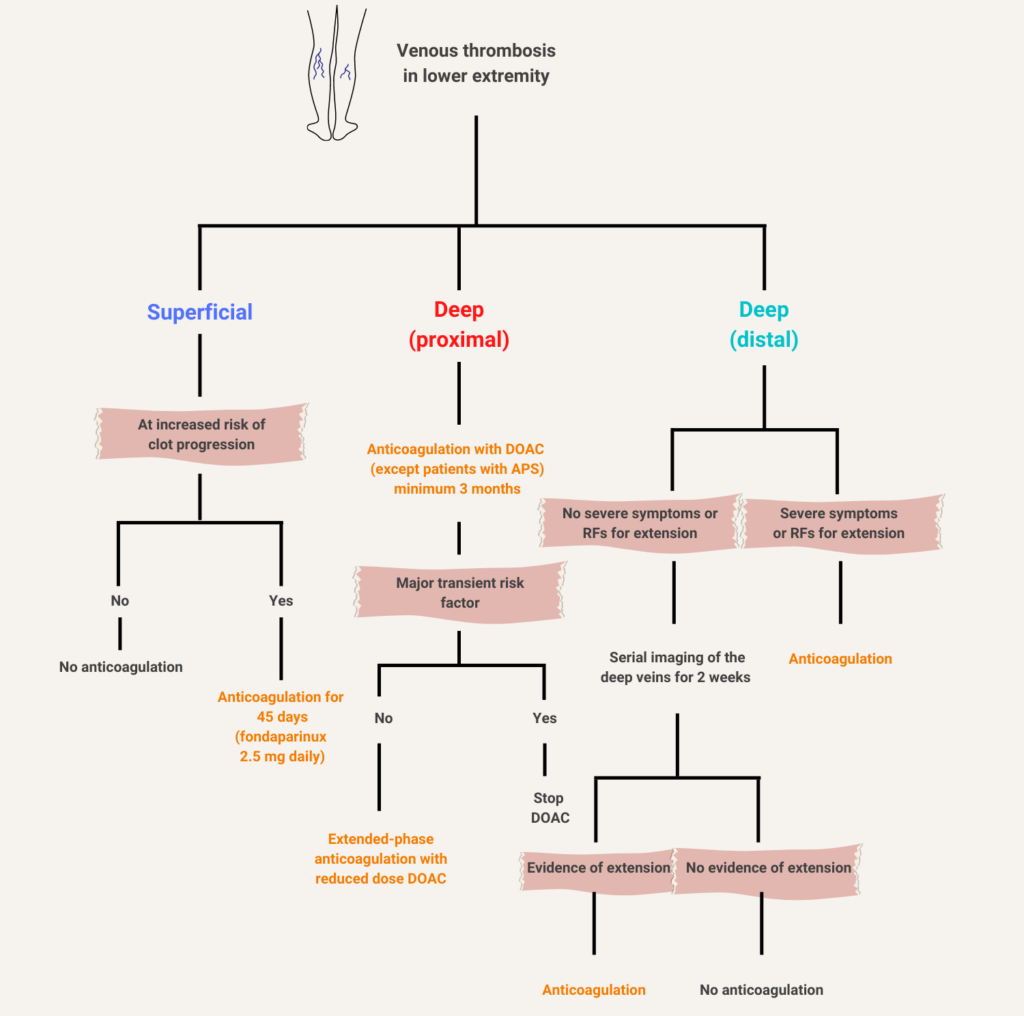
Leg vein thrombosis. In patients with superficial vein thrombosis (SVT), anticoagulation is recommended in those at risk for progression. Factors that favor the use of anticoagulant therapy in patients with SVT include extensive SVT, involvement above the knee, particularly if close to the saphenofemoral junction, severe symptoms, involvement of the greater saphenous vein, history of venous thromboembolism (VTE) or SVT, active cancer, or recent surgery. While fondaparinux (2.5 mg daily) is preferred, rivaroxaban 10 mg daily is a reasonable alternative in patients with SVT who refuse or are unable to use parenteral anticoagulation. Anticoagulation should be given for 45 days. Patients with clinically suspected SVT above the knee should have ultrasonography to exclude proximal DVT. Patients with distal DVT may present with or without severe symptoms or risk factors for extension. Those without symptoms or risk factors for extension may be monitored (no anticoagulation) with serial imaging of the deep veins for 2 weeks. If the thrombus not extend, no anticoagulation is given. If the thrombus extends but remains confined to the distal veins, anticoagulation may be considered. If the thrombus extends into the proximal veins, anticoagulation is strongly recommended. In patients with proximal DVT, anticoagulant therapy with DOAC is recommended (except for patients with confirmed antiphospholipid syndrome, who should be treated with vitamin K antagonist; DOACs must be used with caution in patients with renal insufficiency [creatinine clearance < 30 mL/min] and moderate to severe liver disease). All such patients should receive at least 3 months of anticoagulation. Extended-phase anticoagulation (beyond the initial 3 months) should be offered to patients in the absence of transient provocation. The use of thrombolytic therapy and inferior vena cava filters in proximal DVT is discouraged, though there are very specific patient populations who may benefit. Based on 2021 Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. APS, antiphospholipid antibody syndrome.