Unknown CBC 2
This case is centered around the following twitter thread:
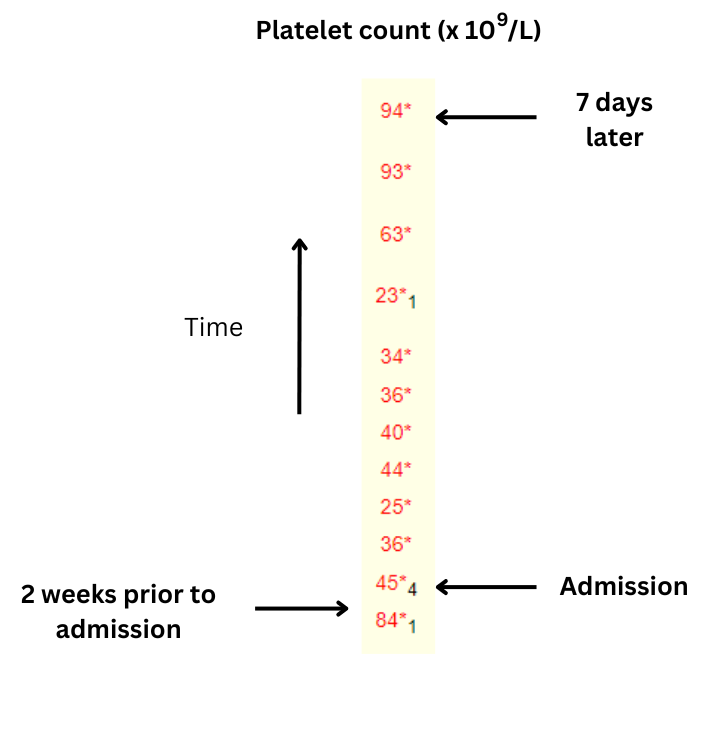
60 yo F presents to hospital with abdominal bloating, macrocytic anemia and thrombocytopenia (see graphic above).
- QUESTIONS:
- How would you explain the drop in Hb over 2 weeks prior to admission?
- How would you explain the sudden normalization of MCV (remember, RBCs survive for 120 days, so there are limited causes for sudden changes in MCV)?
- What do you prefer to use and why: reticulocyte percentage or absolute reticulocyte count?
- Explain the sudden increase in reticulocyte count during hospitalization.
- Finally, what is your overarching diagnosis?
Question 1: How would you explain the drop in Hb over 2 weeks prior to admission?

- Note the significant drop in hemoglobin concentration (Hb) over the 2 weeks prior to admission, and then during hospitalization.
- A reduction in Hb may be explained by one or more of 3 mechanisms:
- Decreased red blood cell (RBC) production
- Increased blood loss
- Increased RBC destruction (hemolysis)
- Without knowing anything else about this case, we can rule out a pure production problem, because even complete bone marrow shutdown would result in only a 1% reduction in red blood cells (and therefore Hb) per day. The numbers don’t add up (see graphic).
- So, there must be some element of blood loss and/or hemolysis.
Question 2: How would you explain the sudden normalization of mean cell volume (MCV) (remember, RBCs survive for 120 days, so there are limited causes for sudden changes in MCV)?

- Any factor that exerts its effect on the bone marrow (at the level of the erythroid progenitor cell) to change red blood cell (RBC) size will have a slow effect on the mean cell volume (MCV) because it takes time to clear the circulating mass of cells with the original size (see graphic).
- A sudden normalization of a previously elevated MCV can be explained by one of 4 mechanisms:
- Loss of reticulocytosis; a classic example is infection with parvovirus B19:
- Parvovirus B19 infects erythroid progenitor cells and causes a transient arrest of erythropoiesis.
- As a result, the reticulocyte count approaches zero.
- In an individual with normal RBC survival, even a complete arrest in RBC production has little effect since the RBC count and Hb only drop by 1%/day, and the infection resolves before a significant, symptomatic drop in Hb occurs.
- In patients with shortened RBC survival (hemolytic anemia) – for example those with sickle cell disease – parvovirus B19 may result in profound anemia.
- Correction of spurious macrocytosis, which may occur in the setting of hypernatremia or hyperglycemia.
- Reversal of an environmental factor that influences RBC size at the level of the mature, circulating RBC. One striking example is the patient with cirrhosis-associated elevation in MCV who has a liver transplant. The MCV correct within 24 hours, providing compelling evidence that macrocytosis associated with chronic liver disease is mediated by plasma factors interacting directly with circulating RBCs (most likely the balance of cholesterol and phospholipids).
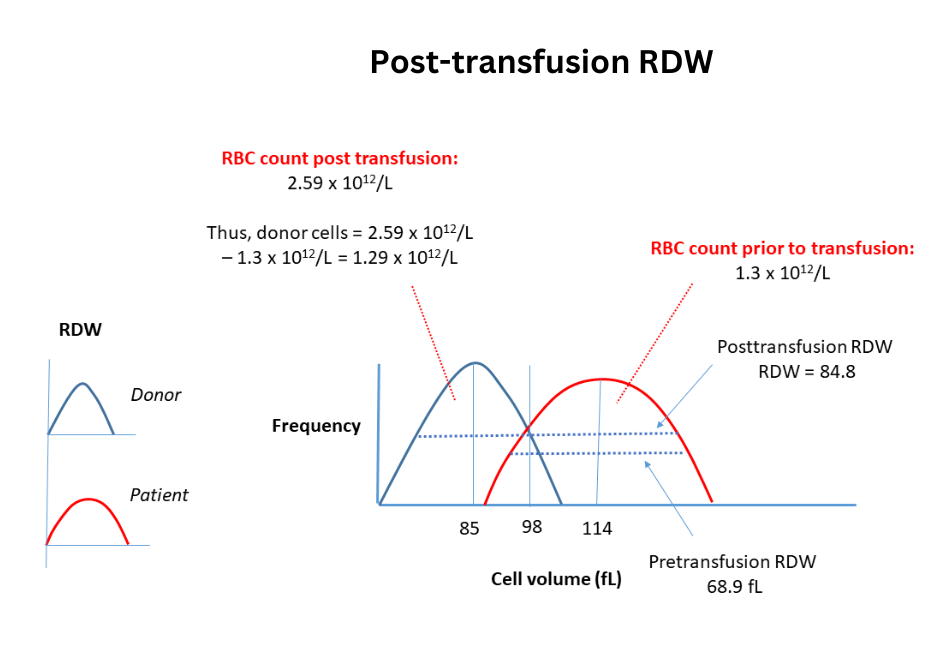
- Red blood transfusion. The vast majority of donors will have normocytic RBCs. When these are transfused in sufficient numbers in patients with macrocytic RBCs, the MCV will shift towards normal levels. The degree of change will depend on the ratio of donor: recipient cell numbers and donor: recipient MCV.
- Loss of reticulocytosis; a classic example is infection with parvovirus B19:
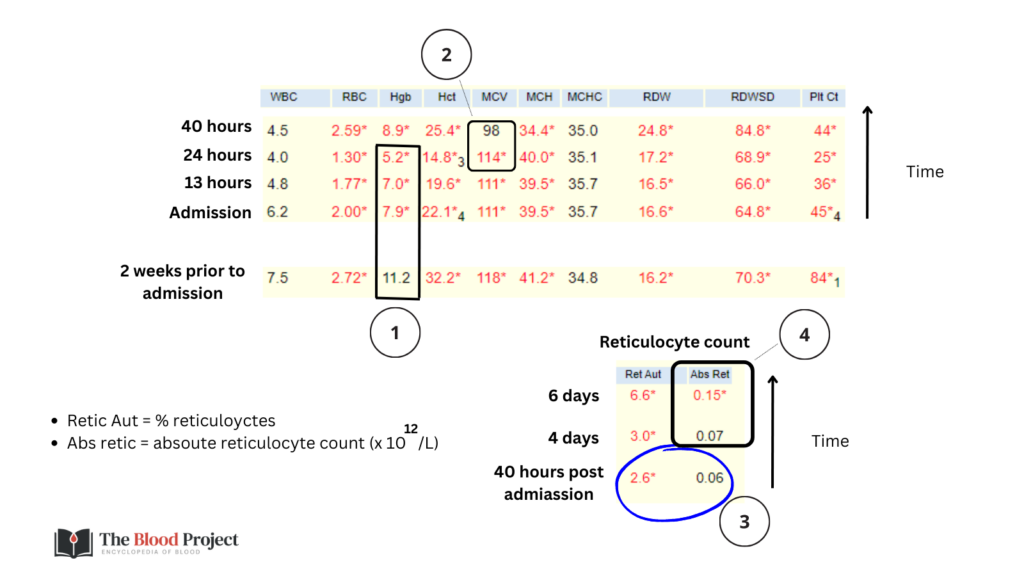
What 2 results in this patient’s CBC favor transfusion as the cause for MCV normalization:
Click for AnswerQuestion 3: What do you prefer to use and why: reticulocyte percentage or absolute reticulocyte count?
For more information on why the absolute retic count is preferred over the retic %, see TBP Tutorial.
Question 4: Explain the sudden increase in reticulocyte count during hospitalization.
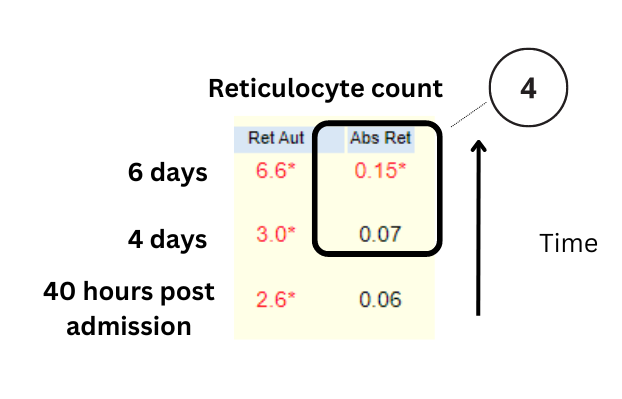
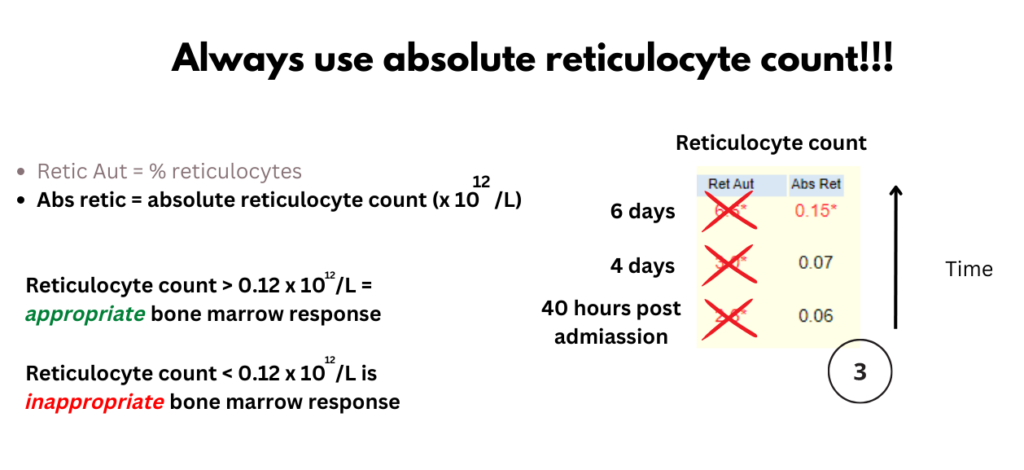
- In this case, the reticulocyte count was inappropriately low 40 hours and 4 days following admission and then appropriately elevated on day 6.
- Anemia with inappropriate reticulocyte count:
- Defined by anemia + absolute reticulocyte count <120 x 109/L or 0.12 x 1012/L.
- Indicates hypoproliferative anemia.
- Categorized as:
- Microcytic
- Normocytic
- Macrocytic
- In this case, the patient presented with hypoproliferative macrocytic anemia. The differential diagnosis includes:
- Megaloblastic causes:
- Vitamin B12 deficiency
- Folate deficiency
- Medication
- Non-megaloblastic causes:
- Liver disease
- Alcohol
- Hypothyroidism
- Primary bone marrow process:
- Myelodysplastic syndrome
- Aplastic anemia
- Plasma cell dyscrasia
- Megaloblastic causes:
- Anemia with appropriate reticulocyte count:
- Defined by anemia + absolute reticulocyte count >120 x 109/L or 0.12 x 1012/L.
- Causes include:
- Blood loss
- Hemolysis
- Erythropoiesis-stimulating agent administration
- In this case, the patient mounted an appropriate reticulocyte count 5-6 days after admission, suggesting one of two possibilities:
- She developed bleeding or hemolysis while in hospital.
- She had bleeding or hemolysis upon admission but erythropoiesis was temporarily suppressed by a factor that was “lifted” during the first days of admission.
What is a classic cause of transient bone marrow suppression associated with macrocytic anemia + thrombocytopenia?
Click for AnswerOverview of case
62 yo F with history of presumed ETOH cirrhosis complicated by portal hypertension, MELD Na score 22, presented with abdominal fullness and discomfort in setting of heavy alcohol use. In addition to her cirrhosis, she has a past history of myocardial infarction and emphysema. Preadmission medications included carvedilol, carisoprodol, and HZT. Physical exam was notable for distended abdomen, non-tender, discomfort to palpation.
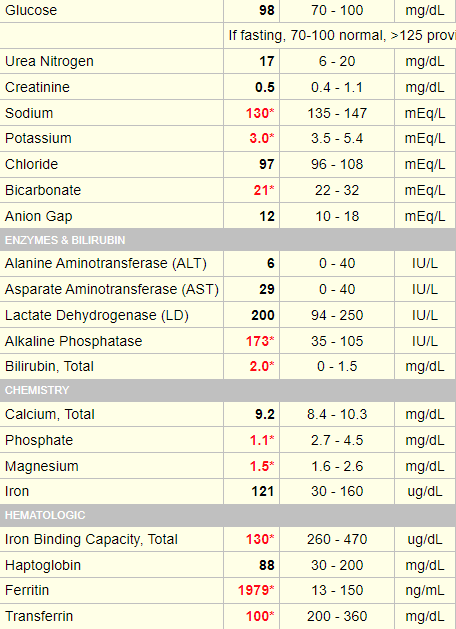
Admission labs:
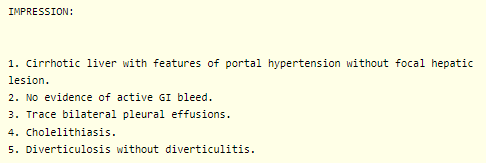
Abdominal ultrasound:

CT abdomen and pelvis:
Course in hospital
The patient was admitted to hospital. Upper endoscopy revealed bleeding esophageal varices, which were banded. She was treated accordingly by the hepatology team. Her Hb stabilized following variceal banding and blood transfusion. Her platelet count eventually increased to her baseline of about 90 x 109/L (see next slide).
Final hematologic diagnosis:
Acute on chronic thrombocytopenia caused by alcohol use and cirrhosis/hypersplenism, respectively. Acute anemia caused by variceal bleed with initial poor reticulocyte response secondary to bone marrow suppressive effects of alcohol. Transient normalization of MCV (with enhanced anisocytosis) secondary to red cell transfusions.