TTP Case 2
Let’s start with the following lab data.

What can you say about this patient (more than one answer may apply)?
a
Likely has aHUS
b
Likely has TTP
c
By definition has TTP
d
Has congenital, not acquired TTP
e
Has HELLP
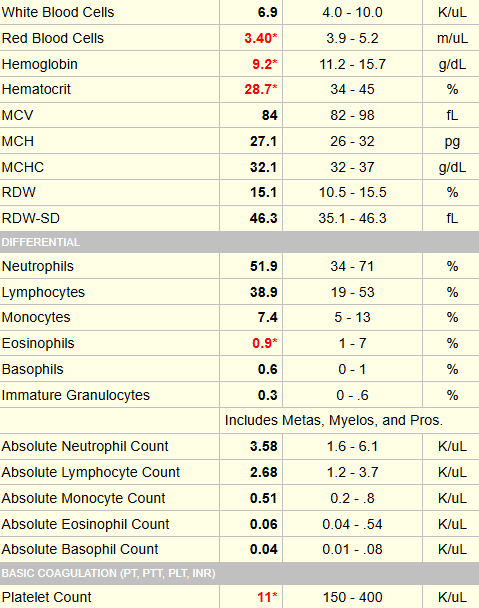
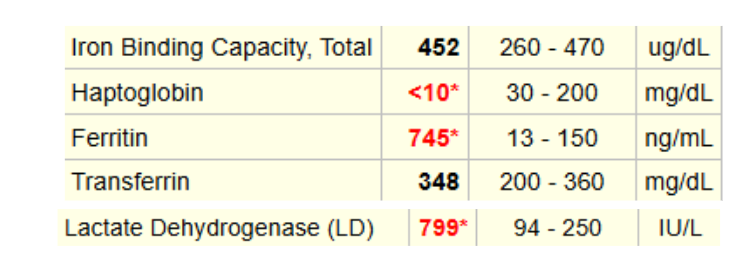
Are these data consistent with hemolysis?
a
Yes
b
No
The smear showed findings similar to the following:



This patient was previously well – no history of cancer or transplantation. If you plug in her data, you end up with a PLASMIC score of 7 (this is the maximum you can have), which is high probability of having TTP.
How do steroids work in TTP?
Click for Answer
