Schistocytes
The following are examples of 4 of the 5 schistocyte types recognized by the Schistocyte Working Group of the International Council for Standardization in Haematology (ICSH):

The presence of schistocytes helps to narrow the differential diagnosis to a thrombotic microangiopathy (TMA), including thrombotic thrombocytopenia purpura (TTP), hemolytic uremic syndrome (HUS) or disseminated intravascular coagulation (DIC).
Can the number/frequency of schistocytes help make a diagnosis of TMA?
- Schistocyte count is up to 0.2% in normal individuals.
- In DIC, the schistocyte count is typically between 0.2% and 1%. However, counts can exceed 1%.
- In TTP and HUS:
- A robust morphological indication for the diagnosis of thrombotic microangiopathic anemia in adults should be recognized when the percentage of schistocytes is above 1%. However, a lack of schistocytes does not exclude a priori the diagnosis of TMA (learn more here). There is no threshold schistocyte number below which the possibility of TTP can be excluded.
- In the appropriate clinical context, more than two schistocytes per high-powered field or more than 1.0% schistocytes on a blood film is considered pathologic; however, these cut-offs have not been validated (learn more here).
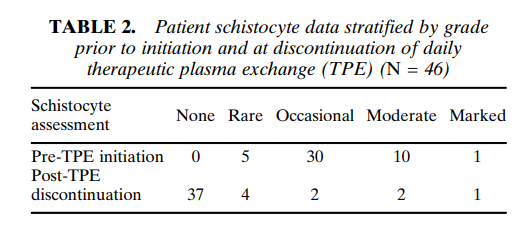
The following are results from a a cohort of 46 patients with TTP and severe ADAMTS13 deficiency. Note the wide variation in schistocyte counts:
Bottom line:
A high number of schistocytes on the peripheral smear suggests a diagnosis of thrombotic microangiopathy (TMA), but cannot reliably distinguish between TTP and other types of TMA.