Quiz – Name that Score!
By William Aird
Data from the original study reporting the HLH-2004 criteria
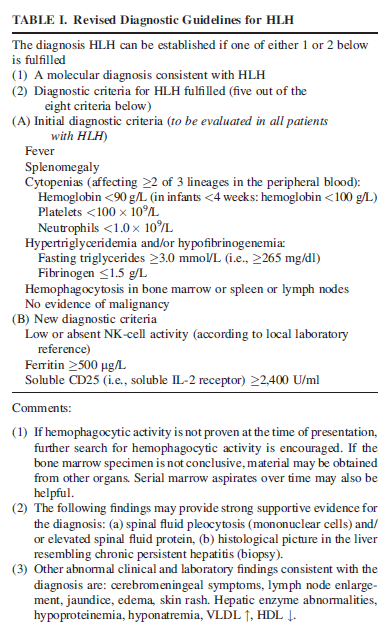
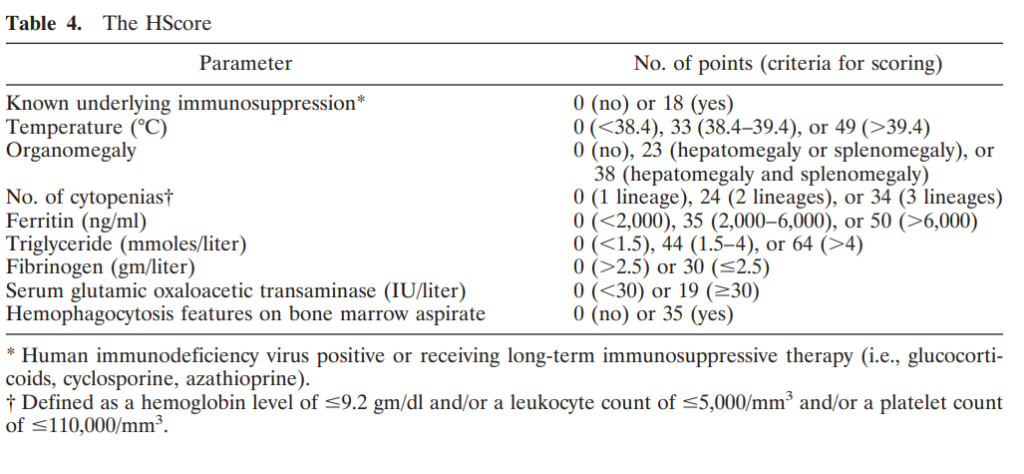
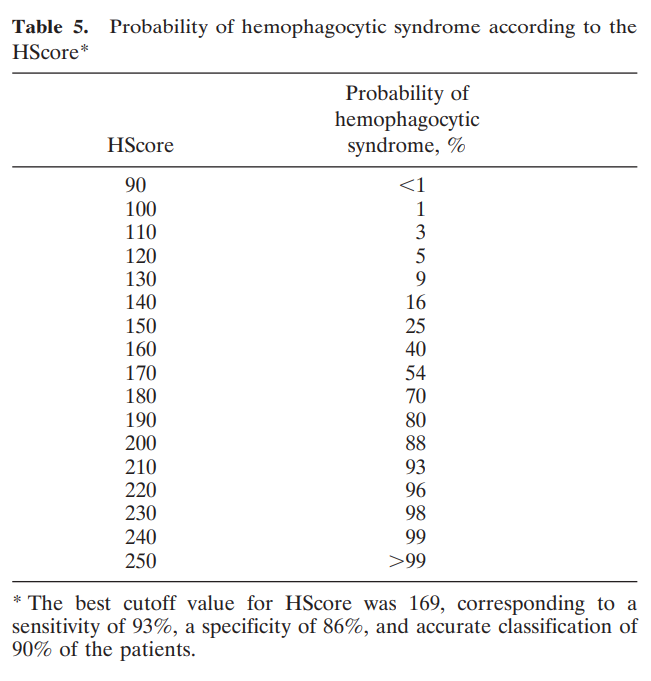
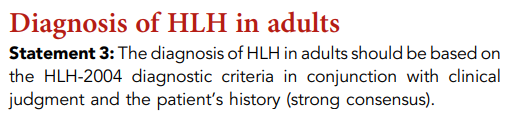
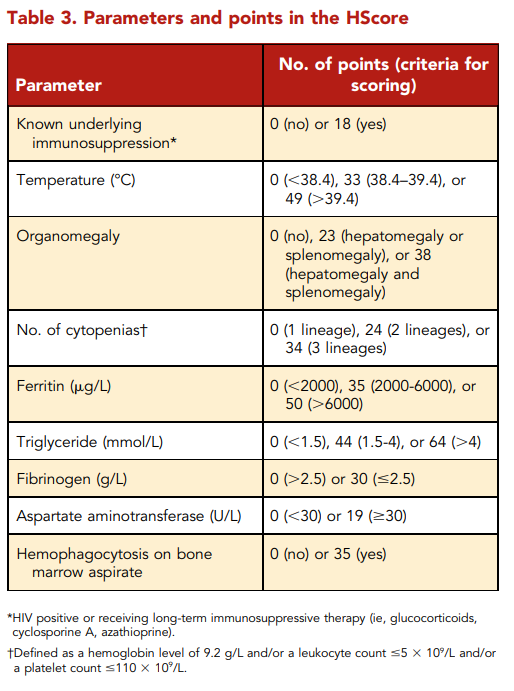
What do the guidelines say about HLH-2004 and the HScore?
Recommendations for the management of HLH in adults, based on expert opinion:

To reiterate, DIC is diagnosed when the ISTH DIC score is 5 or higher:
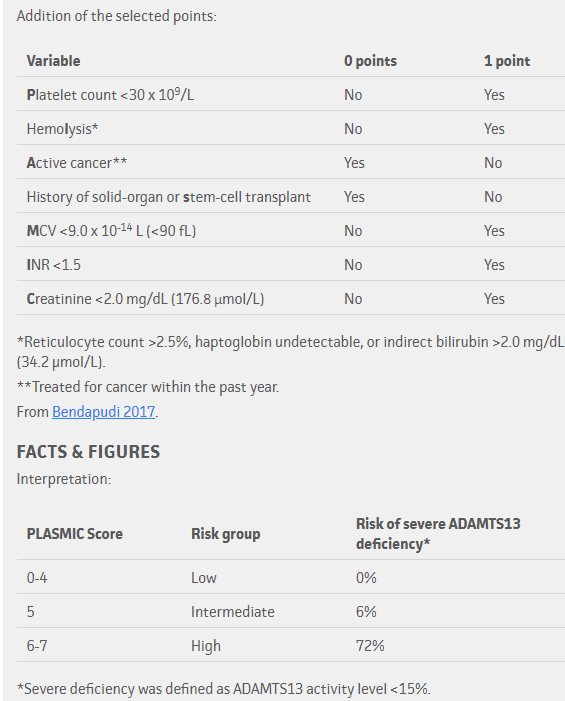
To reiterate, the pretest probability of TTP based on PLASMIC score:
What do the clinical practice guidelines say?
ISTH guidelines for the diagnosis of thrombotic thrombocytopenic purpura:
“The panel agreed that any diagnostic strategy would have to start with a thoughtful assessment of the patient’s pretest probability of having TTP and the use of a formal risk assessment or pretest probability assessment model would not be inappropriate [hardly an enthusiastic endorsement for using a scoring system!]… they noted that both the PLASMIC and the French scores [details of the French score can be found here] were designed for adult populations with no comorbid conditions (eg, pregnancy, cancer, sepsis, organ/tissue transplantation, etc.), which may not be reliable in assessing children and patients with other comorbidities.”
“… in settings with a timely access to plasma ADAMTS13 activity testing and for patients with a high clinical suspicion (≥90% pretest probability) of TTP (eg, based on clinical assessment or a formal clinical risk assessment method), the panel suggests the following diagnostic strategy. (A conditional recommendation in the context of low certainty evidence)”

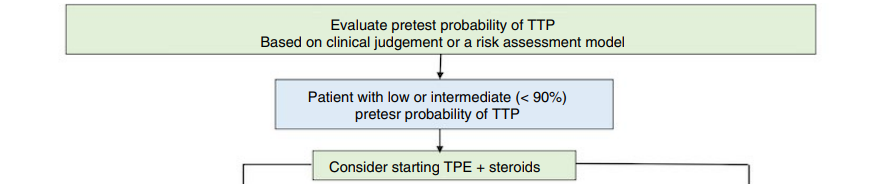
According to these practice guidelines, then, clinical judgement independent of a clinical scoring system, is sufficient for diagnosis. Importantly, the use of a clinical scoring system as the PLASMIC score, has a hugely significant impact on therapeutic decisions.
What are the T’s in the 4T score?
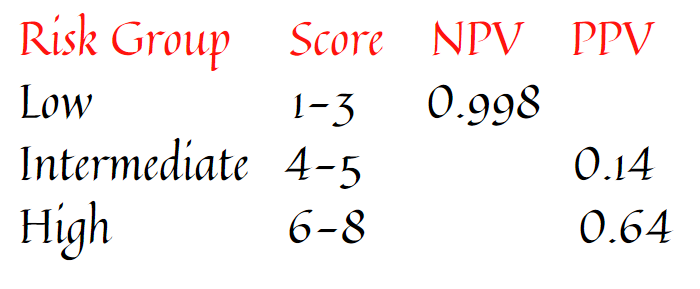
The negative and positive predictive values of the 4T score based on points:
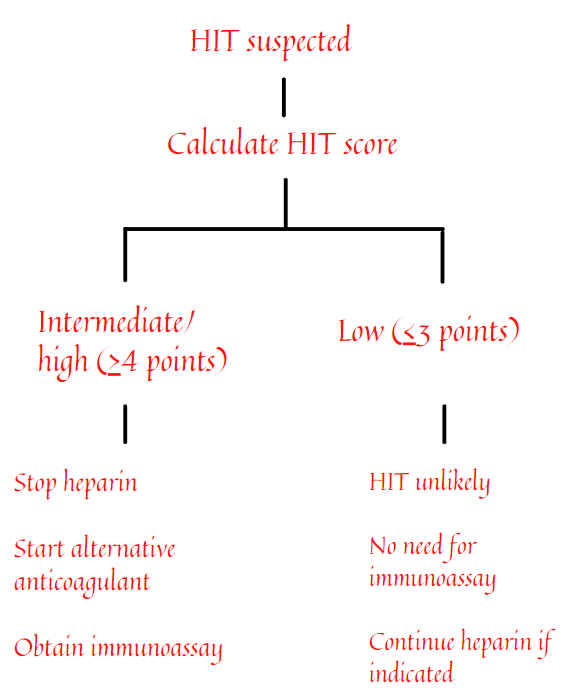
Incorporating the 4T score into a diagnostic and therapeutic algorithm
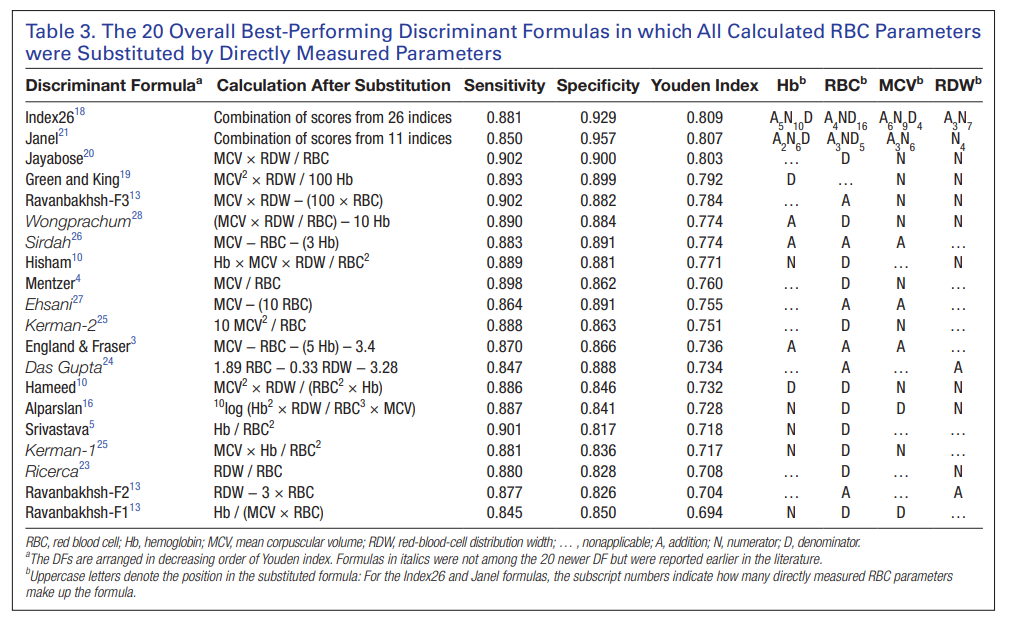
The Mentzer index:

Ratio > 13 suggests iron deficiency anemia; ratio < 13 suggests thalassemia trait
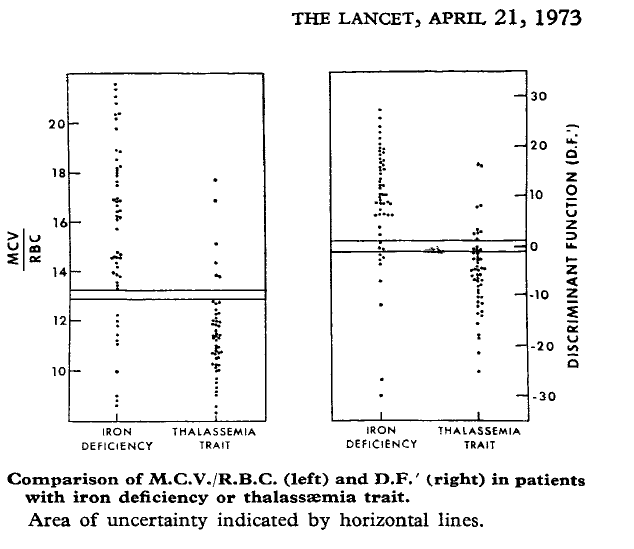
The Mentzer index is just one of many formulas reported to help distinguish between iron deficiency anemia and thalassemia minor!