Postscript
Introduction
- Hyperkalemia is a frequent clinical problem.
- Severe hyperkalemia is a dangerous and life-threatening condition requiring immediate medical intervention.
- Pseudohyperkalemia is an artificial increase in serum potassium due to the release of potassium from tissue or blood cells during or after venipuncture.
- It is important to distinguish true hyperkalemia from pseudohyperkalemia, because immediate recognition of pseudohyperkalemia prevents misdiagnosis and unnecessary intervention, which might lead to iatrogenic hypokalemia. Failure to make the diagnosis may have profound impact on patient safety.
- Pseudohyperkalemia is most commonly induced by fist clenching during phlebotomy, by hemolysis due to mechanical stress during venipuncture, or by prolonged transportation.1
Definition
- In healthy individuals normal serum potassium is defined as levels between 3.5 and 5 meq/L (mmol/L).
- Hyperkalemia:
- Mild, serum potassium ranges from 5.1 to 6.1 meq/L (mmol/L).
- Moderate, serum potassium ranges from 6.2 to 7.0 meq/L (mmol/L).
- Severe hyperkalemia, serum potassium > 7.0 meq/L (mmol/L).
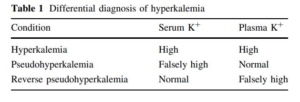
- Pseudohyperkalemia (aka spurious hyperkalemia, factitious hyperkalemia, and artefactual hyperkalemia) is defined as and characterized by marked elevation of serum potassium levels (>0.4 meq/L [mmol/L]) as compared to the normal plasma potassium concentration in the absence of clinical evidence of electrolyte imbalance.
- Serum vs. plasma potassium levels:
- Serum values are always noted to be higher than plasma values because the process of blood clotting when preparing serum is associated with release of potassium from activated platelets.
- The mean difference between serum and plasma potassium levels is 0.36 ± 0.18 meq/L (mmol/L).2
- This difference does not normally exceed 0.4 meq/L (mmol/L).
- Pseudohyperkalemia should only be considered when the serum potassium level exceeds that of plasma by 0.4 meq/L (mmol/L).
- Seasonal pseudohyperkalemia refers to elevations in potassium concentration observed in blood samples drawn in doctors’ offices and transported to the lab in the cold of winter.
- Reverse pseudohyperkalemia is defined as falsely elevated potassium levels in plasma samples as compared to serum, which has been reported in chronic lymphocytic leukemia. Believed to be caused by heparin-induced cell membrane damage during processing (especially during pneumatic tube transport) and centrifugation.
History
- Pseudohyperkalemia first reported by Hartmann and Mellinkoff in 1955:3
- The authors noted that the potassium concentration in a 70 yo man with platelet counts between 1,200,000 and 2,000,000 per cu. mm. (secondary to agnogenic myeloid metaplasia) was markedly elevated in serum obtained from clotted whole blood but not platelet-free plasma. They wrote:
- “These results demonstrated that the apparent elevation of serum potassium concentration actually represented a spurious hyperkalemia“.
- Similar results were obtained in other patients with thrombocytosis.
- The authors concluded that:
- “Some patients with thrombocytosis may have an associated spurious hyperkalemia in the absence of symptoms or signs of hyperkalemia”.
- The high potassium in serum is due to leakage from platelets in vitro during the clotting process.
- The authors noted that the potassium concentration in a 70 yo man with platelet counts between 1,200,000 and 2,000,000 per cu. mm. (secondary to agnogenic myeloid metaplasia) was markedly elevated in serum obtained from clotted whole blood but not platelet-free plasma. They wrote:
- In 1960, Nilsson et al. suggested that potassium could be released from other cellular components and assumed that red blood cells might be the source.
- In 1966 Bronson et al. described 3 cases of pseudohyperkalemia in chronic myelogenous leukemia in transformation and concluded that the white blood cell breakdown could release potassium during coagulation.
Causes
- Common causes include a factors and variables during and after blood collection (release of potassium from muscle from fist clenching while preventing potassium clearance with a tourniquet, long transport time, cooling of blood sample) and by medical conditions associated with a marked increase in the leukocyte, platelet, or erythrocyte count, especially in the context of hematological malignancies that can render the abnormal cells especially fragile.
- Rare causes include genetic defects of cation transport that allow rapid leakage of potassium from erythrocyte after blood drawing.

The American Journal of Medicine (2022) 135:e150−e154
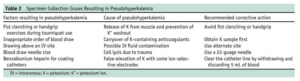
- Preanalytical variables
- Collection technique:
- Fist clenching during phlebotomy:
- Fist clenching during use of a tourniquet is a major cause of pseudohyperkalemia.
- Fist clenching for 1 min during phlebotomy shown to increase potassium levels by as much as 1.0 meq/L (mmol/L).4
- Handgrip exercise shown to raise the plasma potassium concentration by 1.4 meq/L (mmol/L) (with no change in plasma potassium concentration in the samples obtained from the contralateral arm).5
- Tourniquet:
- Prolonged tourniquet time may induce hemolysis and should be minimized to avoid this effect.
- One study showed that application of a tourniquet for more than 1 min caused 20% of the samples to become hemolyzed, while application of tourniquet for less than 1 min associated with a hemolysis rate of only 1.3%.6
- on et al.10 did not observe a significant change of
plasma potassium concentration after application of a tourniquet for 3 m Other studies have shown minimal affect of tourniquet on serum potassium levels.
- Fist clenching during phlebotomy:
- Collection technique:

N Engl J Med. 1990 May 3;322(18):1290-2.
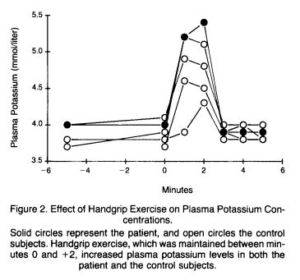
N Engl J Med. 1990 May 3;322(18):1290-2.
-
- Contamination by a potassium-containing substance (e.g. potassium ethylenediaminetetraacetic acid (K-EDTA)):
- The potassium may be transferred from one tube to the next on the tip of the needle when drawing blood.
- To minimize the probability of K-EDTA contamination in serum samples, in guidelines regarding blood collection practices published by several organizations, it has been recommended that serum tubes should be taken prior to K-EDTA containing tubes.
- That being said, the order of blood draw into different tubes has been shown to have only a small effect on serum potassium.7
- Hemolysis:
- Hemolysis during or after phlebotomy is the commonest cause of pseudohyperkalemia.
- The increase in potassium value is correlated with the degree of hemolysis.
- Previous studies have shown that hemolyzed serum or plasma containing 1 g/L of hemoglobin will cause an increase of 0.27–0.33 meq/L (mmol/L) potassium.8
- Causes include:
- Mechanical stress during venipuncture (e.g. excessive vacuum during the blood draw and use of a fine-gauge needle):
- In general, a 21-gauge needle should be selected for drawing blood for serum potassium, and samples for serum potassium should be drawn first.
- Vigorous mixing of the tube.
- Centrifugation at excessive speed.
- Heat exposure in the centrifuge.
- Cold ambient temperatures or prolonged cold storage laboratory conditions, which inhibit the red blood cell Na+-K+ ATPase, which results in cellular K+ leakage artificially raising serum potassium. Cooling blood to 4˚C accelerates the rate at which potassium leaks out of red cells. Maintaining blood sample temperature a few degrees above 20 degrees Celsius will minimize the risk of spurious serum potassium concentration measurements.9
- Delays in specimen transport. A minimum of 30 min is needed to form a blood clot for serum preparation. The maximum recommended time between collection and separation of clot and serum is 2 h.10
- Mechanical stress during venipuncture (e.g. excessive vacuum during the blood draw and use of a fine-gauge needle):
- Contamination by a potassium-containing substance (e.g. potassium ethylenediaminetetraacetic acid (K-EDTA)):
The American Journal of Medicine (2022) 135:e150−e154
- Patient factors
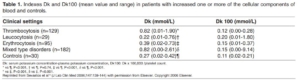
- Thrombocytosis:
- Pseudohyperkalemia reported in patients with primary and reactive thrombocytosis.
- Under normal conditions, potassium concentration in serum is slightly higher than that in plasma (0.36 +/- 0.18 meq/L [mmol/L]) because of the release of potassium from platelets during clotting.
- Previous studies have shown that:
- Platelet counts of >500 × 109 cells/L significantly increase the measured serum vs. plasma potassium concentrations.
- The mean difference between serum and plasma potassium concentration was 0.22 (0.01-0.76) in 29 patients with thrombocytosis.11
- The difference between plasma and whole blood potassium was minimal at all platelet counts.12
- Approximately 14% of serum samples from patients with platelet count >500 × 109 cells/L have a > 1 mEq/L (mmol/L) increase relative to whole blood potassium.13
- There is a significant correlation between platelet count and the difference between serum and plasma potassium values:
- In one study, the magnitude of the increase was approximately 0.05 mEq/L (mmol/L) per each 100 × 109/L increase in platelet count 14
- In another study, elevation of blood platelet count by 1000 × 109/L caused an increase of about 0.2 meq/L (mmol/L) in plasma potassium concentration and 0.7 meq/L (mmol/L) in serum potassium.15
- The incidence of pseudohyperkalemia was reported to be 34% in patients with a platelet count over 500 x 109/L and only 9% if the platelet count was less than 250 x × 109/L, indicating that the serum potassium concentration was directly proportional to the platelet count.16
- Leukocytosis:
- Increased plasma potassium concentration is correlated with leukocyte count.17
- The mean difference between serum and plasma potassium concentration was 0.22 (0.01-0.76) in 29 patients with leukocytosis.18
- The impact of WBC count on the difference between serum and whole blood potassium was about 0.2 mEq/L increase expected with each 100 ×109/L increment in cell count.19
- The impact of the white blood cell count on the difference between plasma and whole blood potassium was 0.6 mEq/L increment expected for every 100 ×109/L increment in count.20
- In patients with white blood cell counts >50 ×109/L, >25% of serum and plasma samples showed a > 1 mEq/L (mmol/L) increase relative to whole blood potassium.21
- Cell fragility in leukocytosis can cause cell lysis exacerbated by centrifugation.
- Vacutainer tubes or syringe shaking were shown to induce lysis of leukemic lymphocytes in patients with chronic lymphocytic leukemia.22
- Erythrocytosis:
- The mean difference between serum and plasma potassium concentration was 0.39 (0.02-0.73) in 95 patients with erythrocytosis.23
- The difference between serum and plasma potassium concentration:24
- Is elevated in patients with erythrocytosis, including those with polycythemia vera and secondary polycythemia, typically:
- > 0.70 meq/L (mmol/L) in polycythemia vera
- < 0.70 in secondary polycythemia
- Inversely correlated with hematocrit
- Is elevated in patients with erythrocytosis, including those with polycythemia vera and secondary polycythemia, typically:
- The potassium load that exits platelets during the clotting process may be diluted in a significantly smaller volume of serum, which results in increased potassium concentration.
- Thrombocytosis:
- Hereditary conditions:
- Isolated familial pseudohyperkalemia (FP) (aka “leaky red cell syndrome”):
- Autosomal dominant condition; individuals are asymptomatic.
- Characterized by temperature-dependent potassium leakage through the red blood cell membrane when stored at room temperature, with a maximum increase at 4 h.
- Circulating plasma potassium concentration is normal.
- Associated with mutation in the ABCB6 gene (2q36), which encodes a membrane protein that is
ubiquitously expressed in human tissues and implicated in porphyrin transport.
- Hereditary stomatocytoses (HSt):
- Group of rare, dominantly inherited hemolytic anemias characterized by macrocytosis and the presence of abnormally shaped red blood cells with abnormal membrane permeability to Na+ and K+
- Patients also have an excessive erythrocyte fragility and excessive K+ leak at lower temperatures.
- Isolated familial pseudohyperkalemia (FP) (aka “leaky red cell syndrome”):
Mechanisms
- Overview of K+ homeostasis:
- The total body potassium concentration in an adult male is approximately 50 mmol/kg of body weight.
- Approximately 98% of the total body potassium is present in the intracellular fluid and only 2% is in the extracellular fluid.
- Intracellular potassium concentration 150–160 meq/L (mmol/L), extracellular potassium concentration of 3.5–5.0 meq/L (mmol/L).
- Most of the intracellular potassium is distributed in muscle; other sites are bone, liver and red blood cells.
- The relationship between extra- and intracellular potassium ion (K+) (the potassium gradient) determines the resting membrane potential and, thereby, the excitability of neurons and muscle cells. Therefore, relatively small changes in the extracellular K+ may have an adverse effect on neuromuscular function, leading to:
- Cardiac arrhythmias
- Skeletal muscle weakness
- Smooth muscle dysfunction causing gastrointestinal upset
- The high intracellular potassium concentration is maintained by the Na+-K+ ATPase pump with slow diffusion of potassium outward via the cell membrane.
- The total body potassium concentration in an adult male is approximately 50 mmol/kg of body weight.
- Serum vs. plasma potassium concentration:
- The potassium concentration in serum is slightly higher than that in plasma because of the
release of potassium from platelets which undergo aggregation and degranulation during clotting. - The mean difference between serum and plasma potassium levels is 0.36 ± 0.18 meq/L (mmol/L).
- The potassium concentration in serum is slightly higher than that in plasma because of the
- Pathophysiology of pseudohyperkalemia:
- The elevation of potassium is due to the release of potassium from cells during the processes of specimen collection and clot formation.
- The elevation in potassium concentration that results from:
- Fist clenching is due to the local release of potassium during contraction of forearm muscles.
- Hemolysis is due to release of potassium from RBCs.
- Elevated blood cell counts is due to release of potassium from the cellular components of blood.
- Release of potassium from the cellular components of blood after collection can occur by rupture
or by increased permeability of the cell membrane. - It is possible that pseudohyperkalemia may occur in cases in where the platelet count is normal but platelets are hyperactivated (for example, in patents in the intensive care unit).
Diagnosis
- Suspect diagnosis in patient with hemolyzed serum sample (readily detected by laboratory analyzers) or with marked leukocytosis or thrombocytosis and a high serum potassium level who lack clinical or ECG evidence of hyperkalemia and have no obvious identifiable cause of hyperkalemia.
- Confirm diagnosis by demonstrating normal potassium level in plasma (collected in lithium heparin) or ABG syringe (whole blood; particularly valuable in the emergency department after normal hours) flushed with heparin (potassium levels measured in whole blood and plasma have been shown to be essentially same).
- Corresponding whole-blood and plasma potassium concentrations are similar.
- Plasma and whole-blood potassium values within the reference interval exclude genuine hyperkalemia.
- In cases of hypokalemia, the same factors that cause pseudohyperkalemia can mask hypokalemia as ‘‘normal-kalemia’’ by falsely raising potassium levels to the reference interval.
Mitigation steps
- Use a 21-gauge needle for drawing blood.
- Draw serum samples first.
- Avoid fist clenching during tourniquet application (the use of tourniquet alone generally does not raise serum potassium).
- Ensure adequate clot formation before centrifugation.
- Avoid long delay between blood collection and centrifugation:
- Analysis within 30 min, if possible.
- The Clinical and Laboratory Standards Institute recommends that samples be centrifuged within 2 h of collection.
- Avoid storage of blood at cold ambient temperatures.
Na+-K+ ATPase