Postscript
Introduction
- Hematological abnormalities are common in patients with chronic liver disease/cirrhosis.
- Alterations include:
- Cellular:
- Red blood cells:
- Macrocytosis
- Anemia
- Platelets:
- Thrombocytopenia
- Alterations in platelet function
- White blood cells:
- Leukopenia
- Neutrophil dysfunction
- Immunosuppression
- Red blood cells:
- Coagulation:
- Changes in all 3 phases of hemostasis:
- Primary hemostasis
- Secondary hemostasis
- Fibrinolysis
- Reduced levels of hepatocyte-derived:
- Procoagulants
- Anticoagulants
- Fibrinolytic proteins
- Increased levels of factors expressed in other cell types (especially endothelial cells), including:
- Factor VIII (FVIII)
- von Willebrand factor (vWF)
- Tissue-type plasminogen activator (t-PA)
- Plasminogen activator inhibitor (PAI-1)
- Historically, the changes in hemostasis that occur in liver disease were assumed to reflect an acquired bleeding disorder (patients were thought to be “autoanticoagulated”). This classical interpretation of the coagulopathy of liver disease has been replaced by the concept of rebalanced hemostasis.
- Changes in all 3 phases of hemostasis:
- Cellular:
- Hematological changes in chronic liver disease/cirrhosis are associated with increased rates of:
- Infection
- Bleeding
- Thrombosis
Definitions
- Hypersplenism is defined as a syndrome that includes:
- Splenomegaly
- Anemia, leukopenia, and/or thrombocytopenia
- Compensatory bone marrow hyperplasia
- Improvement after splenectomy (if performed)
Epidemiology
- Macrocytosis:
- Degree of MCV elevation is greater in those with alcoholic vs. non-alcoholic liver disease
- Macrocytosis reported to occur in:1
- 30% of patients with non-alcoholic liver cirrhosis
- 76% of those with alcoholic liver disease
- Only a subset of patients with macrocytosis also have anemia.
-
Cytopenias:
- Anemia:
- Reported in about:
- 75% of cases overall
- 60% of patients with compensated cirrhosis and portal hypertension
- In one study of 463 participants with hepatitis B-related cirrhosis:
- 66% normocytic anemia
- 27% macrocytic anemia
- 7% microcytic anemia
- Reported in about:
- Anemia:
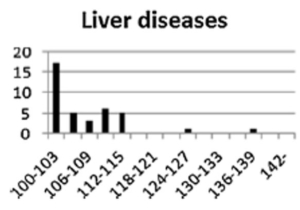
Histograms of MCV in each causative disease from Tohoku University Hospital. The horizontal lines indicate the range of MCV values with a bin width of 3 fL. The vertical lines indicate the number of patients. Note that the MCV is typically <115. Source
.
-
- Thrombocytopenia:
- Reported in about 75% of patients with cirrhosis; of those with thrombocytopenia:
- Mild in 76%
- Moderate in 13%
- Severe in 1%
- Typically mild to moderate; platelet count rarely < 30-40 x 109/L.
- The degree of thrombocytopenia correlates with severity of liver disease:
- 5.5% in patients with stage 0–II fibrosis.
- 64% in patients with stage III-IV fibrosis.
- Reported in about 75% of patients with cirrhosis; of those with thrombocytopenia:
- Leukopenia:
- Typically late onset in patients with cirrhosis.
- Most commonly observed with other cytopenias (anemia, thrombocytopenia, or pancytopenia)
- Cohorts:
- Study of 213 subjects with compensated cirrhosis without esophageal varices followed over time:
- 92% had thrombocytopenia during the study:
- 84% had it at baseline.
- 16% developed it during the course of the study.
- 60% had anemia during the study:
- 37% had it at baseline.
- 63% developed it during the course of the study.
- 55% had leukopenia during the study:
- 42% had it at baseline.
- 58% developed it during the course of the study.
- By the end of the study 92% of those enrolled had thrombocytopenia. In the majority of the individuals this was accompanied by either a bicytopenia or pancytopenia.
- 92% had thrombocytopenia during the study:
- Study of 213 subjects with compensated cirrhosis without esophageal varices followed over time:
- Thrombocytopenia:

- Coagulation abnormalities:
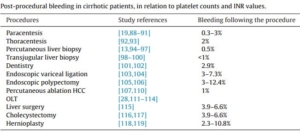
- Rate of bleeding:
- <3% after paracentesis, thoracentesis, and percutaneous or transjugular liver biopsy.
- <10% following endoscopic variceal ligation, endoscopic polypectomy, and minor abdominal surgery (such as cholecystectomy or hernioplasty).
- Portal vein thrombosis (PVT) is the most common venous thromboembolism (VTE) event in cirrhosis:
- Increased rates in the setting of decompensation.
- Incident PVT ranges from 5% at 1 year to 40% at 10 years.2
- Reported incidence of non-portal VTE in patients with chronic liver disease 0.5%-6.7% per year. In a meta-analysis, the cumulative odds ratio for all VTE events was 1.7 for patients with cirrhosis compared to controls.
- Rate of bleeding:
Pathogenesis
- Normal physiology:
- Cellular:
- The liver produces thrombopoietin, the primary physiologic regulator of platelet production.
- Coagulation:
- Liver hepatocytes produce:
- Procoagulant proteins:
- Factor II (FII)
- FV
- FVII
- FIX
- FX
- FXI
- Anticoagulant proteins:
- Antithrombin
- Protein C
- Protein S
- Fibrinolytic components:
- Plasminogen
- Alpha-2-antiplasmin
- Thrombin-activatable fibrinolysis inhibitor (TAFI)
- Procoagulant proteins:
- Hemostatic factors produced by other cell types include:
- Procoagulants:
- Factor VIII (FVIII) – synthesized by endothelial cells in the liver and other selected vascular beds including the kidney.
- von Willebrand factor (vWF) – synthesized by endothelial cells and megakaryocytes.
- Anticoagulants:
- Tissue factor pathway inhibitor (TFPI) – synthesized by endothelial cells.
- Fibrinolytic components:
- Tissue-type plasminogen activator (t-PA) – synthesized by endothelial cells.
- Plasminogen activator inhibitor 1 (PAI-1) – synthesized by endothelial cells.
- Procoagulants:
- Liver hepatocytes produce:
- Cellular:
- Chronic liver disease/cirrhosis:
- Cellular:
- General mechanisms of cytopenias include:
- Portal hypertension/hypersplenism
- Viral infections
- Drugs, including antiviral agents
- Use of alcohol
- Thrombocytopenia:
- Portal hypertension/hypersplenism:
- In patients with cirrhosis, there is a redistribution of platelets, with up to 90% of the circulating platelet mass located in the enlarged spleen (platelet sequestration).
- Platelet counts correlate inversely with spleen size in some but not all studies.
- Finding of thrombocytopenia in patients with cirrhosis is so highly suggestive of the presence of portal hypertension that current endoscopy guidelines use platelet counts as a criterion for gastroesophageal variceal screening.
- Direct splenic destruction of platelets (in addition to platelet sequestration/pooling in the spleen).
- Reduced synthesis of thrombopoietin (TPO):
- TPO:
- Main physiologic regulator of platelet production.
- Produced primarily by the liver (at a fairly constant rate), and to much lesser extent by kidney, muscle and bone marrow.
- TPO mRNA levels are significantly reduced in tissue from cirrhotic livers, and serum TPO levels are lower in patients with cirrhosis.
- TPO:
- Bone marrow suppression, secondary to:
- Viral infection
- Medications such as antiviral therapy
- Alcohol
- Folate deficiency
- Immune-mediated platelet destruction, which may occur in patients with:
- Hepatitis C
- Primary biliary cirrhosis
- Cirrhosis-related hypercoagulability resulting in platelet activation.
- Dilutional thrombocytopenia occurs with volume resuscitation by crystalloid, colloid, or massive blood transfusions.
- Portal hypertension/hypersplenism:
- Platelet function:
- Conflicting data on platelet function in chronic liver disease.
- Reported changes include:
- Defective adherence to injured vessels
- Decreased aggregation
- Reduction in response to signaling stimuli
- Derangements in platelet function reported to worsen with the degree of liver dysfunction and Child-Turcotte-Pugh (CTP) class.
- Additional factors that adversely impact platelet function include:
- Uremia
- Medications
- Sepsis
- Nutritional deficiencies
- Impairments in platelet function may be offset by increased endothelial-derived von Willebrand factor (vWF) in patients with cirrhosis.
- Anemia:
- Acute or chronic blood loss due to variceal or other gastrointestinal bleeding
- Portal hypertension/hypersplenism
- Spur cell anemia
- Zieve syndrome
- Etiologies associated with specific causes of cirrhosis:
- Hepatitis-associated aplastic anemia
- Hemolysis associated with Wilson disease
- Antiviral therapy administered for hepatitis C
- Leukopenia:
- Portal hypertension/hypersplenism
- Viral infection
- Medications such as antiviral therapy
- Alcohol
- Folate deficiency
- General mechanisms of cytopenias include:
- Coagulation:
- Reduced hepatic synthesis of:
- Procoagulant proteins:
- Factor II (FII)
- FV
- FVII
- FIX
- FX
- FXI
- Fibrinogen:
- Levels are normal or increased in most patients with stable cirrhosis.
- 50%-78% of patients with chronic liver disease develop an acquired dysfibrinogenemia in which hepatocytes synthesize an abnormal fibrinogen with increased sialic acid residues, which impair polymerization of fibrin monomers.
- Anticoagulant proteins:
- Antithrombin
- Protein C
- Protein S
- Fibrinolytic components:
- Plasminogen
- Alpha-2-antiplasmin
- Thrombin-activatable fibrinolysis inhibitor (TAFI)
- Procoagulant proteins:
- Non-hepatic synthesis of other coagulation factors:
- Procoagulants:
- FVIII:
- Levels often increased several-fold in patients with stable cirrhosis.
- Increased levels result from increased synthesis in endothelial cells (FVIII is an acute phase reactant).
- FVIII:
- Anticoagulants:
- Tissue factor pathway inhibitor (TFPI) levels are normal or elevated in patients with chronic liver disease.
- Fibrinolytic components:
- Tissue-type plasminogen activator (t-PA) levels are usually elevated due to release by activated endothelial cells and reduced hepatic clearance.
- Plasminogen activation inhibitor 1 (PAI-1) levels are variable and may be normal or increased.
- Procoagulants:
- Low-grade intrahepatic and/or systemic activation of the hemostatic system results in consumption of hemostatic proteins.
- Concept of rebalanced hemostasis:
- Acquired defects in pro-hemostatic pathways are accompanied by acquired changes in anti-hemostatic pathways.
- The concomitant reduction of liver-derived procoagulants and anticoagulants may result in little net change in hemostatic balance in patients with cirrhosis.
- This conclusion is supported by the observation that thrombin generation in patients with cirrhosis is not different from healthy controls (despite clearly abnormal conventional coagulation tests such as the INR).
- However, the new balance is considered to be precarious with increased sensitivity to small perturbations as occurs with changes in volume status, systemic infection, and renal function.
- American Association for the Study of Liver Diseases (AASLD) Guidance:
- Distinct hypercoagulable and hypocoagulable features may be present simultaneously in an individual patient and may contribute to thrombosis or bleeding, respectively.
- Reduced hepatic synthesis of:
- Cellular:

Clinical manifestations
- Patients with cirrhosis may experience both bleeding and thrombotic complications.
- Bleeding:
- Portal hypertension-related bleeding complications:
- Especially variceal bleeding
- Typically unrelated to coagulopathy
- Provoked bleeds during procedures:
- Especially:
- Paracentesis
- Liver biopsy
- Results from mechanical injury to vessels, not hemostatic failure per se.
- Especially:
- Spontaneous or unprovoked bleeds that may be related to hemostatic failure, including:
- Bruising
- Mucosal bleeding
- Oozing from puncture sites
- Risk factors for bleeding include:
- Advanced portal hypertension
- Acute decompensation of cirrhosis
- Acute-on-chronic liver failure (ACLF)
- Systemic inflammatory response and association with concurrent infection
- Acute kidney injury
- Chronic kidney disease
- Medications, in particular antiplatelet therapy and anticoagulation
- Portal hypertension-related bleeding complications:
- Bleeding:
-
- Thrombosis:
- Types include:
- Portal vein thrombosis and mesenteric vein thrombosis:
- Despite the reduction in platelet number and function, patients with advanced liver disease have an increased risk of thrombotic events, particularly in the portal circulation where blood flow velocity is reduced.
- Non-portal venous thromboembolism (VTE)
- Portal vein thrombosis and mesenteric vein thrombosis:
- Types include:
- Thrombosis:
Diagnosis
- Complete blood count (CBC) may show:
- Leukopenia
- Anemia
- Macrocytosis (MCV > 100 fL)
- MCV in the cirrhotic patients is almost always < 120 fL
- Thrombocytopenia – platelet count rarely < 30-40 × 109/L
- Peripheral blood smear may show:
- Macrocytes
- Target cells
- Spur cells (acanthocytes)
- Coagulation tests:
- Changes in common coagulation assays, including prothrombin time (PT) and partial thromboplastin time (PTT) are sensitive to reduced levels of procoagulants, but not anticoagulants, giving a false impression that patients with cirrhosis are auto-anticoagulated.
- Prothrombin time (PT) and activated partial thromboplastin time (aPTT):
- PT and aPTT do not fully reflect the derangement in hemostasis in liver disease (they do not measure the deficit of liver-derived anticoagulant, such as protein C and S) and do not reliably predict the risk of bleeding, for example at the time of invasive diagnostic procedures:
- Guidelines for liver biopsy acknowledge that there is no specific PT/INR cutoff at or above which bleeding complications can be reliably predicted.
- According to the Italian Association of the Study of the Liver/Italian Society of Internal Medicine (AISF/SIMI):
- Current evidence does not support the use of PT/INR value as a predictor of bleeding or to monitor the effectiveness of anticoagulant therapy in patients with cirrhosis.
- American Association for the Study of Liver Diseases (AASLD) guidance on liver biopsy (2009):
- Decision to perform liver biopsy in patients with abnormal coagulation tests should be reached as the result of local practice(s) and consideration of the risks and benefits of liver biopsy since there is no specific PT, INR, or platelet count threshold for reliably predicting adverse bleeding.
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Simultaneous changes in procoagulant and anticoagulant pathways in patients with cirrhosis result in complex hemostatic changes that are not adequately captured by traditional laboratory measures of hemostasis, such as PT, aPTT, and platelet count.
- INR was developed to standardize PT reporting for patients on stable anticoagulation with vitamin K antagonists (VKA) and is not validated for patients with liver disease. There is significant interlaboratory variability of the INR in patients with cirrhosis, especially at high INR values.
- PT and aPTT do not fully reflect the derangement in hemostasis in liver disease (they do not measure the deficit of liver-derived anticoagulant, such as protein C and S) and do not reliably predict the risk of bleeding, for example at the time of invasive diagnostic procedures:
- Global tests of hemostasis:
- Thrombin generation tests (TGTs):
- Measure thrombin generation +/- added soluble thrombomodulin, which downregulates thrombin generation by increasing activation of protein C.
- While TGTs are better measurements of hemostatic balance than the PT and aPTT, they are not widely available and have not yet been shown to predict risk of bleeding or clotting in liver disease.
- According to the Italian Association of the Study of the Liver/Italian Society of Internal Medicine (AISF/SIMI):
- Thrombin generation assays are promising laboratory tools which may help stratify patients with cirrhosis at risk for hemorrhage or thrombosis.
- Thrombin generation assay with/without thrombomodulin or Protac might be useful to assess the risk for venous thromboembolism in patients with cirrhosis.
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Global tests of hemostasis, such as thrombin generation or whole-blood viscoelastic tests, better capture the general hemostatic status of a patient with cirrhosis, but have not been clinically validated.
- Viscoelastic elastic tests:
- Whole blood tests are collectively known as “viscoelastic elastic tests” and include:
- Thromboelastography [TEG]
- Rotational thromboelastometry [ROTEM]
- Sonorheometry
- These tests depend on changes in a “resistance to motion” measure (TEG, ROTEM) or ultrasound density (sonorheometry) that detect thickness of an evolving clot.
- Whole blood tests offer potentially better means of simulating the in vivo activity of the hemostatic pathways.
- Although traditional laboratory measures of coagulation such as PT and aPTT may suggest a bleeding tendency, whole-blood viscoelastic tests such as TEG or ROTEM, have shown that patients with cirrhosis have normal to elevated thrombin-generating capacity and near-normal whole-blood clot formation.
- the Italian Association of the Study of the Liver/Italian Society of Internal Medicine (AISF/SIMI) recommendations:
- The use of algorithms based on ROTEM/TEG may facilitate targeted transfusions with hemostatic agents, such as fresh frozen plasma, in patients undergoing liver transplantation or in those with severe bleeding.
- The threshold values of these tests to target transfusion requirement need to be established in appropriate clinical trials.
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Global tests of hemostasis, such as thrombin generation or whole-blood viscoelastic tests, better capture the general hemostatic status of a patient with cirrhosis, but have not been clinically validated.
- According to the AGA Clinical Practice Update (2019), the following procedures do not routinely require coagulation assessment in patients with cirrhosis before their performance:
- Diagnostic and therapeutic paracentesis
- Common forms of thoracentesis
- Upper endoscopy to screen for and band esophageal varices
- Diagnostic (but not therapeutic) colonoscopy
- Whole blood tests are collectively known as “viscoelastic elastic tests” and include:
- Thrombin generation tests (TGTs):
Treatment
- Thrombocytopenia:
- Management of periprocedural thrombocytopenia:
- Patient factors to consider include:
- Severity of thrombocytopenia
- Presence or absence of concomitant coagulopathy
- Use of antiplatelet agents or anticoagulants
- Prior history of bleeding with procedures
- Procedure-specific factors include type of procedure
- In vitro data have been interpreted to suggest that platelet levels >55 x 109/L improve hemostasis in
patients with cirrhosis; however:- These in vitro data have only assessed platelet procoagulant activity and have not accounted for potential compensation by von Willebrand factor (vWF) and other endothelial-derived components.
- This threshold has not been validated clinically.
- Platelet thresholds according to procedure:
- Endoscopy:
- Guidelines do not provide exact threshold for upper endoscopy.
- Studies suggest diagnostic upper endoscopy can be safely performed at platelet counts > 20 x 109/L.
- However, some endoscopists prefer platelet counts > 50 x 109/L for endoscopic biopsies.
- For lower endoscopy, many endoscopists use the same parameters as upper endoscopy.
- Paracentesis (diagnostic and/or therapeutic):
- Low risk for bleeding (1 per 1,000 patients).
- Guidelines do not suggest routinely correcting thrombocytopenia before paracentesis.
- Liver biopsy (percutaneous):
- Percutaneous liver biopsy has a higher risk for bleeding compared with paracentesis (severe bleeding in one per 2,500-10,000 cases).
- Typical threshold is platelet count > 50 x 109/L. However, as shown in the table below, the latest AASLD clinical practice guideline recommends against routine pre-procedure correction.
- Endoscopy:
- Patient factors to consider include:
- Management of periprocedural thrombocytopenia:
-
-
- Treatment options:
- Platelet transfusion:
- Expected increase in platelet counts following transfusion with a standard unit dose:
- Approximately 30 × 109/L within 10 minutes of transfusion in patients without cirrhosis.
- Approximately 12 × 109/L within in patients with cirrhosis.
- Consider platelet transfusion when platelet count < 50-60 × 109/L for liver biopsy.
- Risks include:
- Transfusion reactions
- Transfusion reactions
- Cost and logistics
- Expected increase in platelet counts following transfusion with a standard unit dose:
- TPO receptor agonists:
- Peptide TPO agonists:
- Romiplostim (Nplate):
- Injected subcutaneously.
- FDA approved for:
- Patients with immune thrombocytopenia (ITP).
- Patients with hematopoietic syndrome of acute radiation syndrome.
- Not FDA approved for use in patients with nonimmune-mediated thrombocytopenia in chronic liver disease.
- Small studies and case reports exist in patients with liver disease.
- Safety concerns for portal vein thrombosis (PVT) have been raised.
- Eltrombopag (Promacta):
- Oral administration
- FDA approved for:
- Treatment of thrombocytopenia in patients with persistent or chronic immune thrombocytopenia.
- Treatment of thrombocytopenia in patients with hepatitis C infection:
- Boxed warning: In patients with chronic hepatitis C, PROMACTA in combination with interferon and ribavirin may increase the risk of hepatic decompensation.
- Treatment of Severe Aplastic Anemia
- Associated with increased risk of PVT and hepatotoxicity, thus no longer commonly used in patients with liver disease.
- Nonpeptide TPO agonists:
- Two such agents have been approved for increasing platelet counts in patients with cirrhosis:
- Avatrombopag
- Lusutrombopag
- Each requires completion of a 2-to 8-day course preceding the scheduled procedure.
- Both agents have been shown to be superior to placebo in achieving a target platelet count ≥50,000/μL before the procedure, with no statistical differences in thrombotic complications compared to placebo.
- Per American Association for the Study of Liver Diseases (AASLD) Practice Guidance: “Of note, there were no statistical differences in postprocedural bleeding events in these studies between treatment arm and placebo, and therefore routine use of these agents to prevent procedure-related bleeding cannot be recommended.”
- Avatrombopag (Doptelet):
- Oral administration
- FDA approved for:
- Treatment of thrombocytopenia in patients with chronic liver disease.
- Treatment of thrombocytopenia in patients with chronic immune thrombocytopenia (ITP).
- Recently approved for use in patients with advanced liver disease and
thrombocytopenia who undergo elective procedures - Approval based on ADAPT-1 and ADAPT-2 trials.
- Platelet counts rapidly rise after 5 days of avatrombopag, peak at day 10, and return to baseline levels by about 1 month.
- Lusutrombopag (Mulpleta):
- Two such agents have been approved for increasing platelet counts in patients with cirrhosis:
- Romiplostim (Nplate):
- Peptide TPO agonists:
- Splenic embolization or surgical splenectomy:
- these procedures are debatable and not widely recommended.
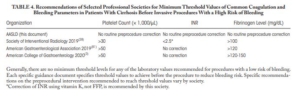
- American Association for the Study of Liver Diseases (AASLD) Practice Guidance:
- Because of conflicting data in the literature, there is no data-driven specific INR or platelet cutoff in which procedural bleeding risk is reliably increased.
- Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low- and high-risk procedures without prophylactically correcting the platelet count.
- An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.
- Platelet transfusion:
- Treatment options:
-
- Coagulation abnormalities:
- Anticoagulant medications should be discontinued prior to liver biopsy.
- Consider stopping antiplatelet medications up to 10 days before liver biopsy.
- In patients undergoing invasive procedures, routine use of fresh frozen plasma (FFP) or coagulation factor concentrates (prothrombin complex concentrate or recombinant factor VIIa [rFVIIa]) based on the prothrombin time (PT) value or the PT-derived INR for primary prophylaxis prior to invasive procedures is not recommended.
- Fresh frozen plasma:
- Infusion of FFP may improve or normalize some coagulation parameters in patients with cirrhosis; however FFP is not routinely recommended because :
- High volumes, which are needed to correct PT/INR, are potentially unsafe.
- Potential for developing transfusion-related lung injury syndromes.
- Increases in portal pressures directly proportional to the volume transfused.
- Minimal efficacy in improving thrombin generation capacity in vitro.
- Clinical benefit has not been established.
- There is no specific PT/INR (and/or platelet count cutoff) at or above which potentially adverse bleeding can be reliably predicted.
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance: “FFP transfusion before procedures is associated with risks and no proven benefits… we advise against prophylactic FFP transfusion before common procedures and await studies with clinically relevant endpoints to yield further guidance.”
- rFVIIa administration:
- Shortens the PT in patients with cirrhosis, but has no proven clinical benefit.
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance: “Its use in a prophylactic setting before invasive procedures is not recommended, and the use of this agent in non-hemophilia patients has been associated with increased risks of thrombosis, including arterial thromboses.”
- Cryoprecipitate or fibrinogen concentrate
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Low fibrinogen levels have been associated with increased bleeding risk in critically ill patients with
cirrhosis. - Correction of plasma fibrinogen to levels >100 mg/dL using cryoprecipitate or fibrinogen concentrate before high-risk procedures could be considered for patients with cirrhosis, but data to support this strategy reducing bleeding complications are lacking.
- Cryoprecipitate and fibrinogen factor replacements are low-volume products effective at increasing fibrinogen levels.
- Low fibrinogen levels have been associated with increased bleeding risk in critically ill patients with
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Vitamin K:
- Routine administration of vitamin K is not recommended to increase the plasma levels of coagulation factors in patients with cirrhosis.
- AASLD: outside of advanced malnutrition states or chronic cholestasis, vitamin K replacement has no measurable effect on the INR in patients with cirrhosis.
- Desmopressin:
- Desmopressin use is not recommended in patients with cirrhosis undergoing elective surgery or at the time of variceal bleeding
- American Association for the Study of Liver Diseases (AASLD) 2020 Practice Guidance:
- Because of conflicting data in the literature, there is no data-driven specific INR or platelet cutoff in which procedural bleeding risk is reliably increased.
- Identification and correction of modifiable risk factors for bleeding before performing procedures, particularly high-risk elective procedures, is recommended. Such risk factors include the use of antithrombotic drugs, acute kidney injury, and infection.
- Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking vitamin K antagonists.
- Infusion of FFP may improve or normalize some coagulation parameters in patients with cirrhosis; however FFP is not routinely recommended because :