ITP – Classification
This patient has a presumed diagnosis of immune thrombocytopenia (ITP). Let’s step back for a moment and consider classification schemes for ITP.
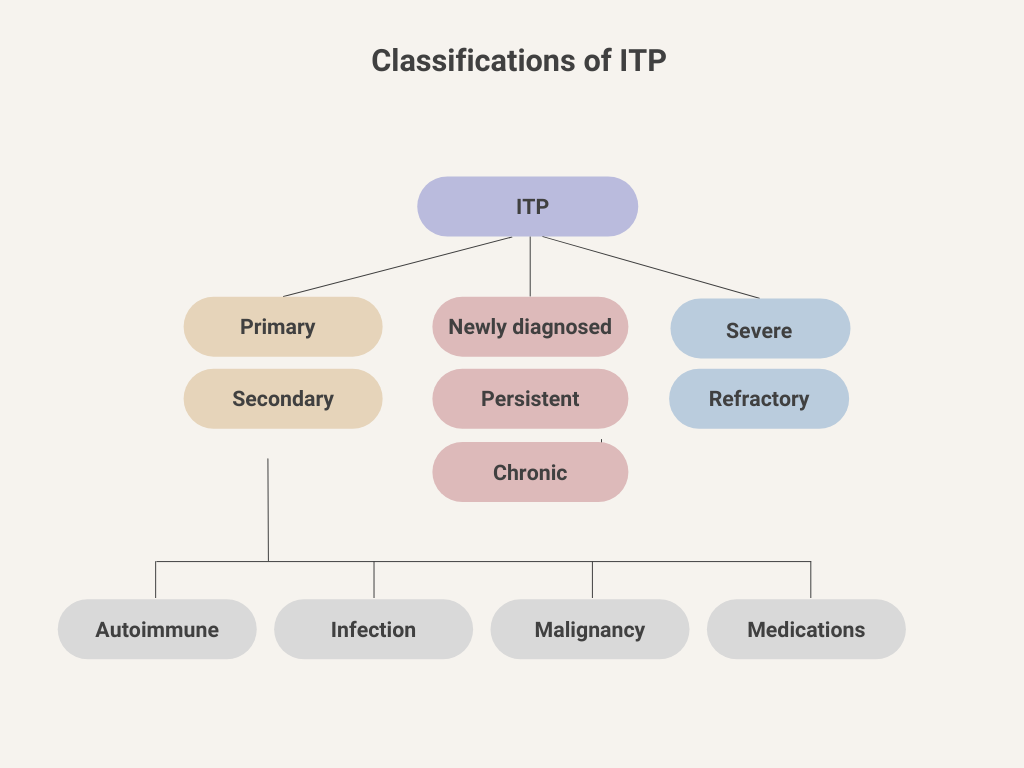
1) Based on underlying cause:
- Primary
- 80% of cases.
- ITP without an obvious initiating or underlying cause.
- International working group: “Primary ITP is an autoimmune disorder characterized by isolated thrombocytopenia (peripheral blood platelet count <100 × 109/L) in the absence of other causes or disorders that may be associated with thrombocytopenia. The diagnosis of primary ITP remains one of exclusion; no robust clinical or laboratory parameters are currently available to establish its diagnosis with accuracy. The main clinical problem of primary ITP is an increased risk of bleeding, although bleeding symptoms may not always be present.”
- Secondary
- 20% of cases.
- ITP due to an underlying disease or drug exposure, including:
- Autoimmune disease – for example, systemic lupus erythematosus.
- Infection – for example, hepatitis C, HIV, and Helicobacter pylori.
- Malignancy – for example, chronic lymphocytic leukemia.
- Medications – drug-induced thrombocytopenia (heparin-induced thrombocytopenia maintains its own designation and acronym (HIT) because of its unique features.)
- International working group: All forms of immune-mediated thrombocytopenia except primary ITP.
2) Based on chronicity:
- Newly diagnosed ITP – ITP diagnosed within last 3 months.
- Persistent ITP – disease duration 3-12 months.
- Chronic ITP – disease duration > 12 months.
3) Based on severity:
- Severe ITP:
- Requiring any disease-directed treatment for clinical bleeding manifestations.
- International working group: “Presence of bleeding symptoms at presentation sufficient to mandate treatment, or occurrence of new bleeding symptoms requiring additional therapeutic intervention with a different platelet-enhancing agent or an increased dose”.
- Refractory ITP – those requiring additional medical treatment following splenectomy or (now that splenectomy is rarely performed for ITP) patients who have failed multiple lines of therapy.
See case study.