Treatment

To summarize at this point, we have a 72 year-old woman with an extremely elevated Hct (polycythemia) who presents with gouty arthritis of her left elbow, and possible symptoms of hyperviscosity (fatigue, “brain fog”). There are no obvious causes of secondary polycythemia, and her complete blood count and differential show concomitant leukocytosis and thrombocytosis, with basophilia – all consistent with a diagnosis of polycythemia vera.
The erythropoietin level eventually returned low, and most importantly the Jak2 V617F mutation ultimately returned positive, securing the diagnosis.
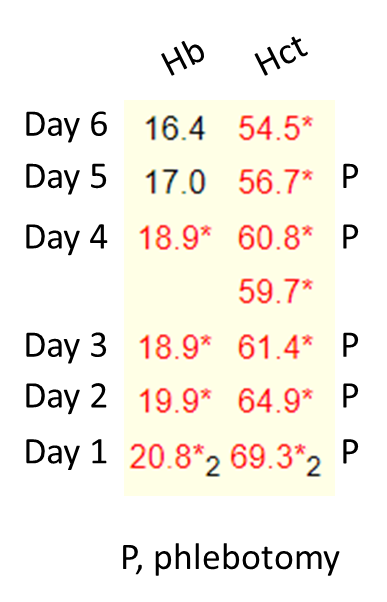
The patient was treated with daily phlebotomy. The response in hemoglobin (Hb) and hematocrit (Hct) is shown below: