History

A 72 year-old woman presented to her PCP with swelling and pain of her left elbow. A history revealed that she had been feeling unusually tired for the past 2-3 months, and she felt she was experiencing “brain fog” with difficulty concentrating and intermittent memory loss. A complete blood count (CBC) was performed and revealed an elevated Hct of 69.3%. She was promptly instructed to go to the emergency department for further work-up. In addition to the symptoms of elbow pain, fatigue and “brain fog”, she tells you that she has noted the palms of her hand to be redder than usual. She has also had several episodes of dizziness after showering over the past 6 months. She denies facial plethora, difficulty with vision, headache, bleeding, easy bruising, fevers, night sweats or change in weight. She has no other active medical problems. There is no family history of elevated Hct or other hematological conditions. She is a non-smoker and denies any alcohol intake. She is a retired restaurant worker. She is not taking any medications and has no known drug allergies.
A good history includes important negatives and positives. The history above mentions dizziness with showering.
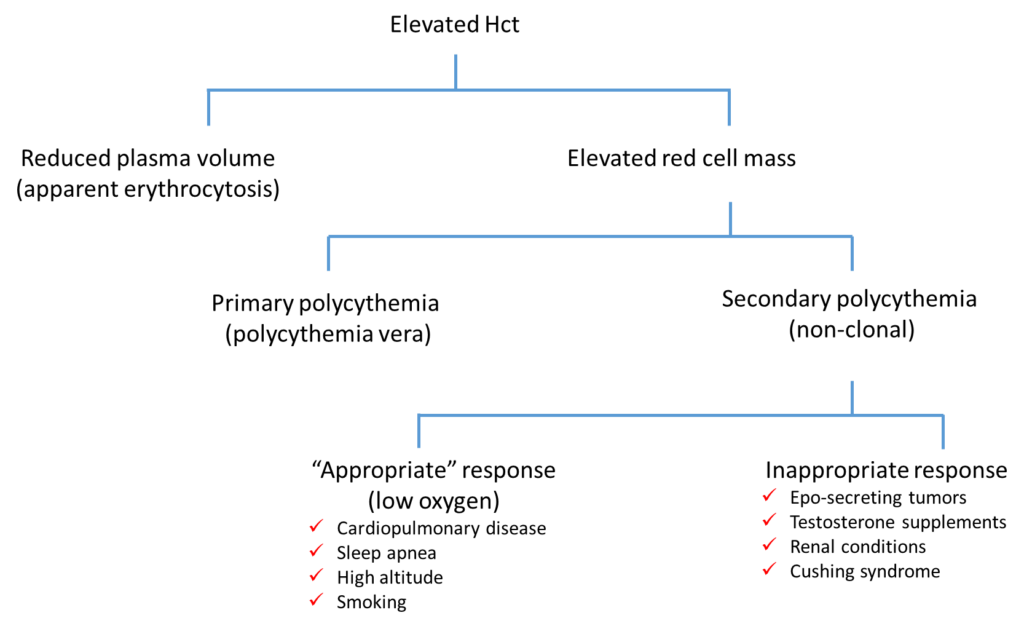
To properly evaluate the appropriate positives and negatives on history, we need to consider the differential diagnosis of an elevated Hct and work our way backwards.