45 yo F with Anemia, Thrombocytopenia and AKI
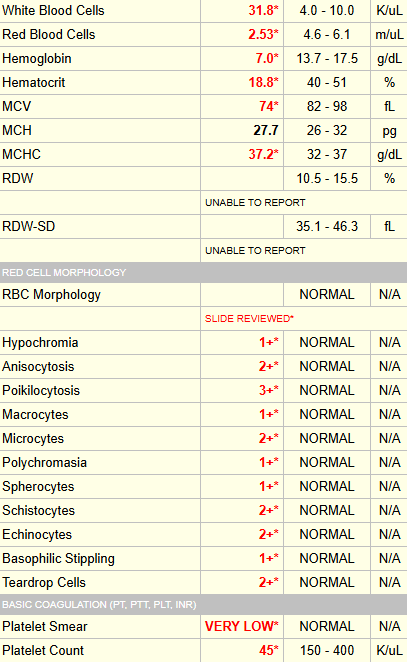
The schistocyte’s, as read out by the lab technician above, were confirmed by the hematology consult team.
Here are some additional labs at presentation:
- Creatinine 4.1
- CRP 186
Note how the MCV was low on transfer and then increased over time to normal values.

This patient scored 6 (out of 7) on the PLASMIC score (she lost a point for the elevated creatinine).
The patient was treated with:
- Therapeutic plasma exchange – a total of 19 daily exchanges until platelet count > 150 x 109/L x 2 days
- Corticosteroids
- Caplacizumab
ADAMTS13 activity level and inhibitor screen came back 6 days later, consistent with acute iTTP:

