Iron overload
We established in the Labs section that the patient’s iron indices are consistent with iron overload:
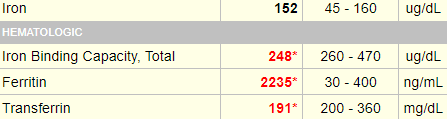
There are many reasons for an elevated ferritin. To test your memory from a previous question, what parameter(s) in this iron panel points to iron overload as a cause?
a
The ferritin is >2000
b
The serum iron is high
c
The total iron binding capacity (TIBC) is low
d
The transferrin saturation (TSAT) is elevated
20%-50% is considered normal; > 50% indicates possible iron overload.
In addition to blood transfusion, what else is contributing to the patient’s iron overload?
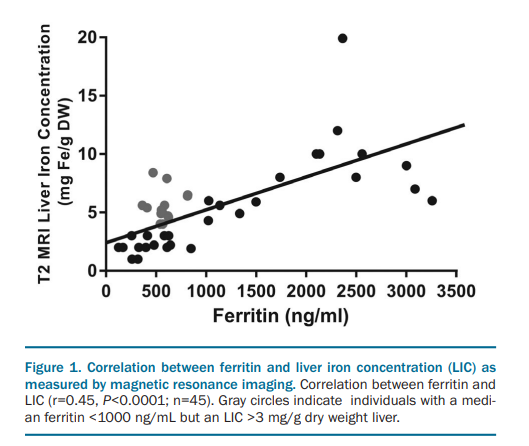
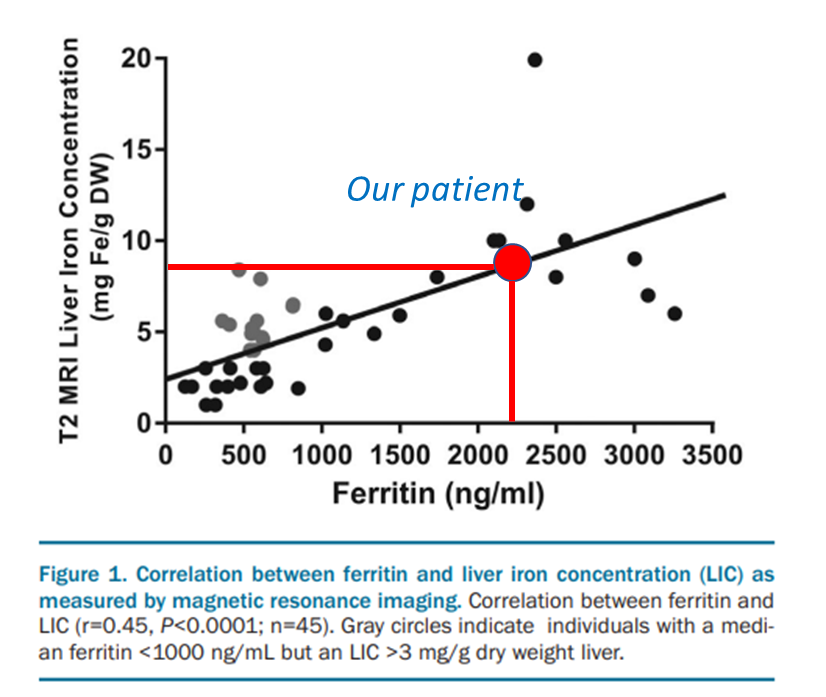
Click for AnswerThe following study demonstrated a correlation between serum ferritin and liver iron concentration in patients with pyruvate kinase deficiency.
Our patient (red circle) had a ferritin of about 2250 ng/ml, which would predict for an LIC of about 8 mg/g DW.
The patient had an MRI of the liver, which showed:

Liver iron concentration (LIC):
- Normal LIC ranges from 0.17-1.8 mg iron/g dry weight.
- < 7 mg iron/g dry weight may not be associated with adverse effects.
- > 15 mg iron/g dry weight associated with:
- Expansion of the chelatable iron pool and labile plasma iron levels.
- Liver fibrosis, liver dysfunction, endocrinopathies, cardiac iron accumulation, and mortality (in patients with thalassemia major).
149 micromoles per gram = 8.3 mg per gram – very close to what was predicted on the last slide.