Labs
Labs (1 of 40 slides)
Labs (2 of 40 slides)
The following is the complete blood count (CBC) at the time of admission:
| WBC (109/L) | Hb (g/dL) | MCV (fL) | PLT (109/L) |
|---|---|---|---|
| 6.6 | 12.7 | 79 | 224 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45%, platelets (PLT) 150-450 x 109/L
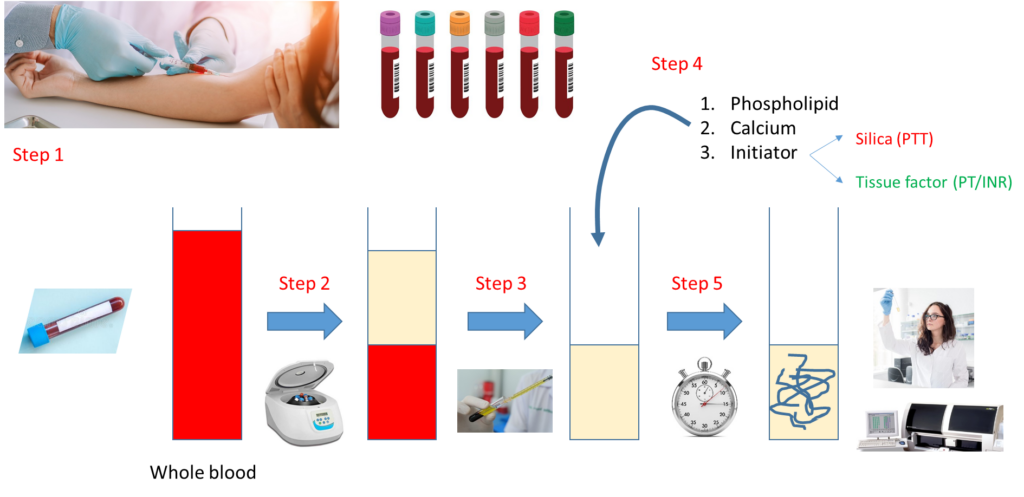
Let’s look at how a PT and aPTT are carried out:
Notes:
- Step 1 – Draw whole blood from a blood vessel (typically an arm vein) into a blue top tube containing the anticoagulant, sodium citrate.
- Step 2 – Spin the liquid blood sample in a centrifuge so that red cells layer on the bottom, plasma on the top.
- Step 3 – Pipette plasma (top layer) into a clean, empty test tube.
- Step 4 – Add phospholipid, calcium and activator (tissue factor for PT, silica for aPTT).
- Step 5 – Incubate at 37 degrees C and measure time to clot formation, either with machine or more rarely by vision.
Note that the major difference between the PT and aPTT is the nature of the activator added to the sample.
A factor IX level was ordered:

The results are expressed as % of normal, which is equivalent to units per deciliter (U/dL) or international units (IU) per deciliter when quantitated by comparison to an international plasma standard. HB is defined as severe if FIX activity is less than 1% (<1 U/dL), moderate if the level is 1–5% (1–5 U/dL), and mild if the level is greater than 5% but less than 40% (>5 to <40 U/dL), although some sources use <50% rather than <40% to define the hemophilia range
Labs (2 of 40 slides)
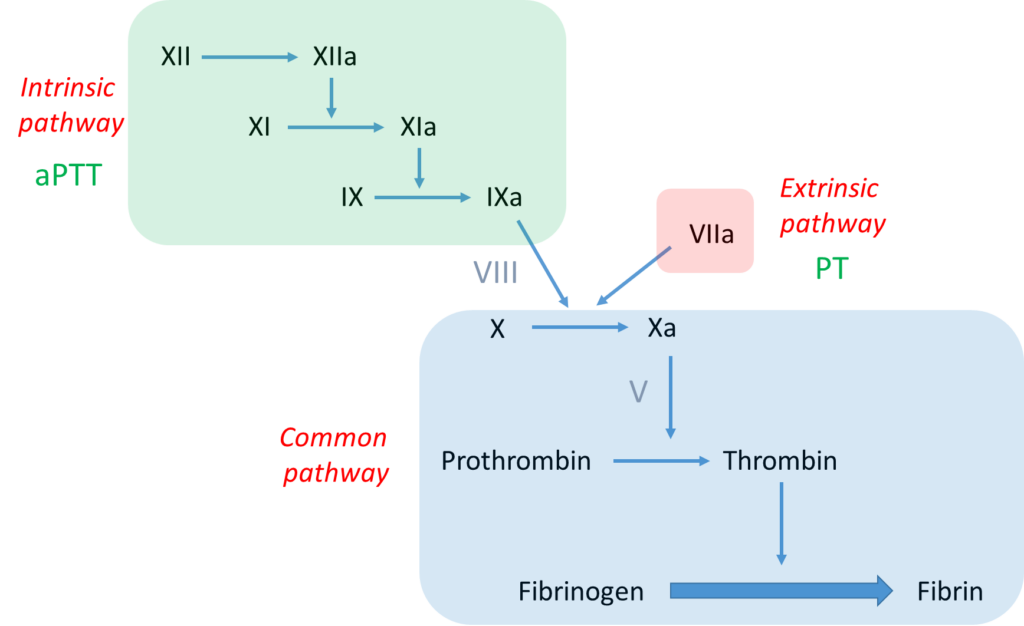
Let’s take a look at where FIX lies in the clotting cascade. It is a serine protease in the intrinsic pathway and mediates the activation/cleavage of FX. FVIII is a cofactor that accelerates the function of FIX.
Note:
- The bottom line is formation of an insoluble fibrin plug, which, along with platelets, stems blood loss.
- Fibrin is derived from thrombin-mediated cleavage of soluble fibrinogen.
- Thrombin (which is a serine protease) is formed when another serine protease, activated factor X (Xa), cleaves prothrombin.
- Two pathways that activate factor X:
- the intrinsic pathway, which consists of a series of linked reactions involving serine proteases FXII, FXI and FIX, and cofactor FVIII
- the extrinsic pathway, which consists of tissue factor-mediated activation of FVII (FVIIa)
- In vivo, the clotting cascade is always initiated by tissue factor activation of FVII (extrinsic pathway) and amplified by the intrinsic pathway via cross-talk (FVIIs activates FIX) and feedback (thrombin activates FXI and FVIII) mechanisms.
- aPTT measures the integrity of the intrinsic pathway.
- PT/INR measures the integrity of the extrinsic pathway.

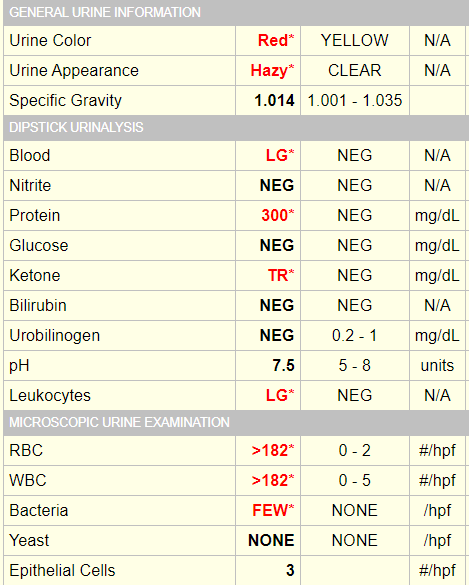
A urinalysis was performed: