
Answers to Case
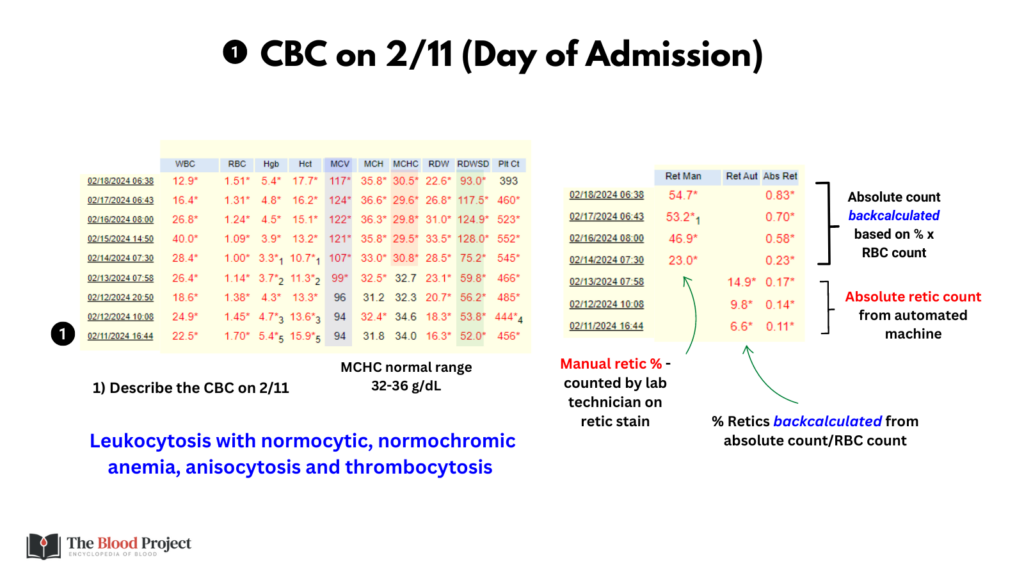
Q1. Describe the CBC on 2/11.
A1. Leukocytosis (WBC > 11 x 10^9/L) with normocytic, normochromic anemia (Hb < 12-13 g/dL, MCV 80-100 fL, MCHC 32-36 g/dL), anisocytosis (RDW-SD > 46 fL) and thrombocytosis (PLT > 400 x 10^9/L).
Q2. Why does the MCV increase?
A2. There are only two ways to acutely increase the MCV above normal: reticulocytosis and in vitro artifact. In this case, the retic count is increasing, accounting for the new macrocytosis.

Q3. Why does the MCHC fall?
A3. Because retics have a lower MCHC than mature RBCs (Hb content/weight per cell does not change as the RBC matures, so it gets more concentrated as the cell gets smaller).

Q4. Why does the RDW increase?
A4. Anisocytosis owing to a mix of retics (which are larger than mature RBCS) and smaller mature RBCs.

Q5. Estimate the size of the patient’s reticulocytes
A5. About 150 fL (see graphic for details)

Assuming a mean reticulocyte volume of 150 fL and a mature RBC mean cell volume of 90 fL, calculation of the predicted MCV on the various dates matches quite well with the actual MCV.
… this was a case of hyperhemolysis in sickle cell disease.
