Localization Before Diagnosis: A Physiology-First Approach to Anemia
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
When clinicians encounter anemia, the reflex is often to ask: What causes this? The instinct is understandable. Medicine trains us to think in diagnoses. But physiology asks a different first question:
Where is the failure occurring?
Anemia is not fundamentally a diagnosis. It is a physiologic disturbance. And physiologic states are best understood not by naming them, but by localizing them. Diagnosis is not the beginning of reasoning. It is the endpoint of successful localization.
Two ways clinicians actually reason
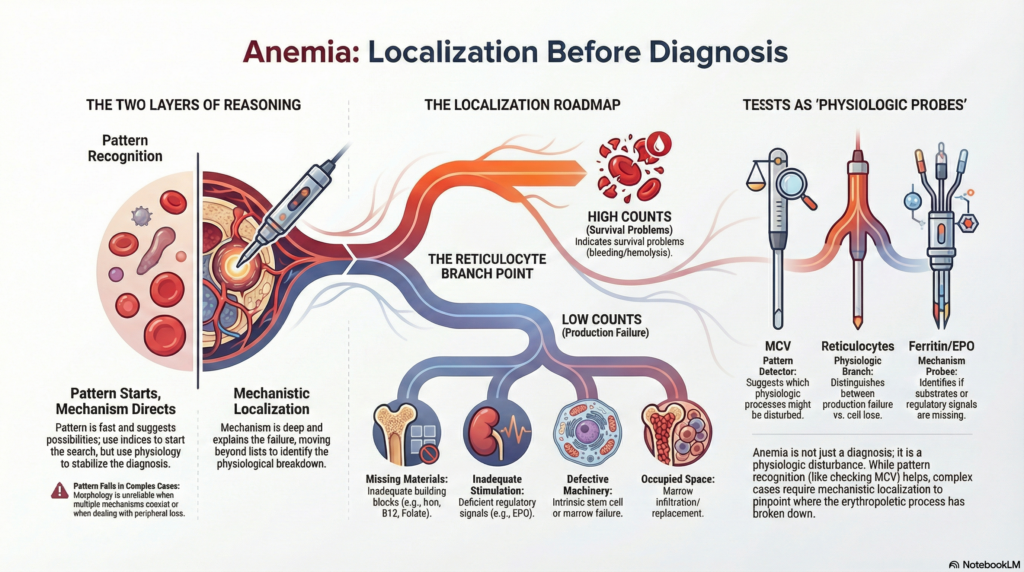
In practice, clinicians use two complementary modes of reasoning when approaching anemia. One is morphologic pattern recognition. The other is mechanistic localization. These are not competing strategies. They are layers of the same reasoning process.
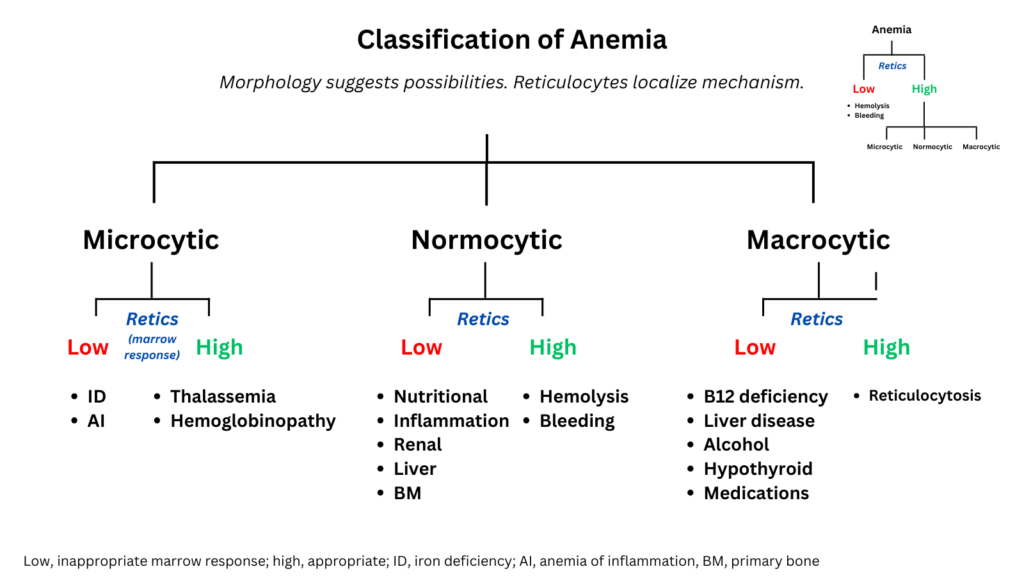
Morphologic pattern recognition is the most visible layer. A low MCV prompts iron studies. A high MCV prompts B12 testing. A normal MCV shifts attention toward inflammation, kidney disease, or marrow disorders. This approach is fast, efficient, and usually correct. Many patients can be evaluated and treated successfully using morphology-guided reasoning alone. Because indices are immediately available, this is often the entry point, especially in general practice.
Mechanistic reasoning operates at a deeper level. Instead of asking what the pattern looks like, the clinician asks where erythropoiesis is failing. Are building components missing? Is stimulation inadequate? Is the marrow itself defective? Is the marrow environment compromised? These questions organize disease by physiology rather than by appearance. In experienced hands, this level of reasoning is often implicit. Hematologists frequently localize mechanism without consciously labeling the step, because training has made physiologic thinking automatic. Teaching, however, requires making that implicit step visible.
Clinical entry points therefore differ. Many clinicians begin with morphology because it is immediately available and often sufficient for common cases, while others begin with reticulocytes to localize physiology first. The physiology is identical in both approaches. Only the starting question differs.
Pattern recognition suggests possibilities. Mechanistic reasoning stabilizes them. Pattern is fast. Mechanism is explanatory. Together they form a single integrated diagnostic process.
Why pattern works so well
Pattern‑based reasoning succeeds most of the time because common diseases present in common ways. Iron deficiency produces microcytosis. Vitamin B12 deficiency produces macrocytosis. Inflammation produces normocytic anemia. When the pattern is classic and the problem is single‑cause, morphology points efficiently toward the right tests.
That is why many clinicians can evaluate anemia effectively without explicitly invoking mechanistic categories. The pattern itself is often sufficient to guide testing and treatment.
Acknowledging this is not a concession. It is simply an honest description of clinical reality.
The traditional framework deserves credit
The classic morphologic approach to anemia, often associated with Wintrobe’s classification, is not a relic. It works because it reflects real biology. Cell size is not arbitrary. It encodes information about hemoglobin synthesis, DNA replication, and marrow kinetics. Clinicians who begin with morphology are not avoiding physiology. They are using a visible surrogate for physiologic processes.
The limitation is not that morphology is wrong. It is that morphology is incomplete. Pattern recognition is an excellent entry point, but it is not a full explanation. Mechanistic reasoning does not replace the morphologic approach. It completes it.
At the bedside, morphology is often the fastest path forward. Conceptually, mechanism is the deepest. Good clinicians learn to move between the two.
Where pattern alone breaks down
Pattern recognition is powerful but fragile. It works best when:
- the presentation is typical
- the disease is common
- only one process is present
Morphology is a map of production, not a monitor of survival.
Pattern recognition is therefore most reliable when anemia reflects impaired production and least reliable when it reflects blood loss or destruction.
When red cell production is impaired, morphology often mirrors the underlying disturbance because cell formation itself is altered. But when anemia results from peripheral loss, morphology may appear deceptively ordinary. Reticulocytosis can raise MCV slightly, yet this signal is inconsistent and easily missed. Without first asking whether marrow response is appropriate, morphology alone may mislead. What appears normocytic may in fact be a highly active marrow responding appropriately to loss.
Pattern recognition also becomes unreliable when:
- multiple mechanisms coexist
- findings conflict
- the presentation is atypical
- the disease is rare
In those situations, lists fail and physiology becomes essential. The question is no longer “What does this look like?” but “Where is the failure?”
That shift from appearance to mechanism is the pivot from pattern recognition to localization.
At this stage, “mechanism” refers only to the physiologic domain of failure. The specific cause of impaired production, such as missing substrate, inadequate stimulation, intrinsic marrow dysfunction, or marrow displacement, is a deeper layer of mechanistic reasoning that comes next.
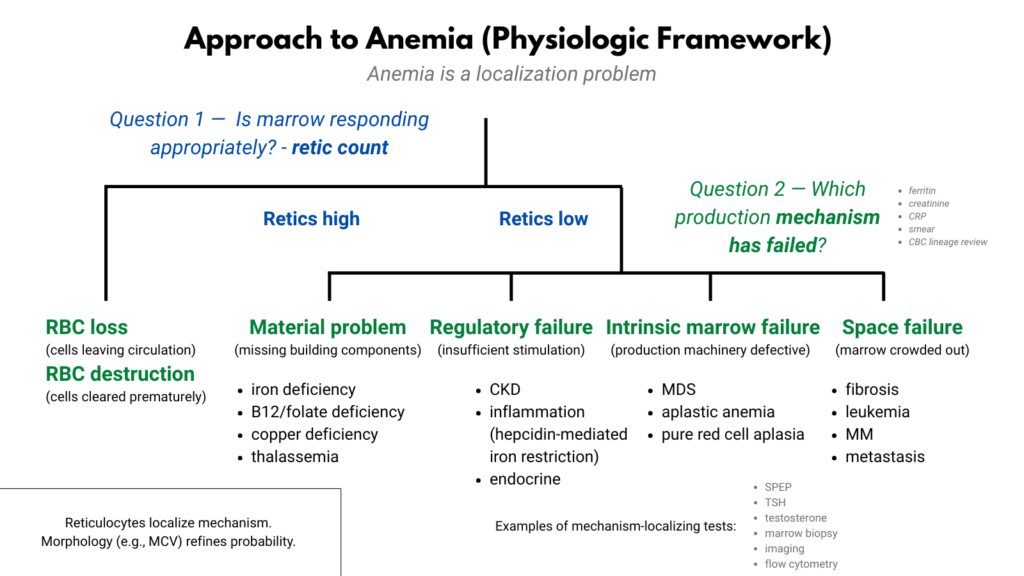
The physiologic branch point
The first true localization step in anemia is the reticulocyte response. Hemoglobin reflects a balance between red cell production and red cell survival. Reticulocytes distinguish which side of that balance is disturbed.
An elevated reticulocyte count indicates appropriate marrow compensation. The anemia therefore arises from premature loss of circulating cells, either through bleeding or destruction.
A low reticulocyte count indicates inadequate production. The problem lies somewhere along the erythropoietic pathway.
Before any diseases are named, the disorder has already been localized to a physiologic domain.
Not all tests serve the same intellectual purpose. Some localize physiology. Some identify mechanisms. Some name diseases. The reticulocyte count, for example, is a localization test: it tells us whether marrow response is appropriate, not what disease is present.
Other tests function at the mechanistic level. Ferritin reveals substrate availability. Erythropoietin reflects regulatory signaling. Testosterone exposes endocrine stimulation. These do not merely label disorders. They explain why red cell production is failing.
And then there are bridge tests, findings that connect levels of explanation at once. A low testosterone level, for instance, identifies both a mechanism, insufficient erythropoietic stimulation, and a disease state, hypogonadism. A low ferritin level provides another example: it simultaneously reveals a mechanism (iron-restricted erythropoiesis) and identifies a disease state (iron deficiency). These are the most educational results in medicine because they link physiology to diagnosis.
The most powerful tests therefore do more than name disease. They reveal the structure of the problem.
How clinicians actually use reticulocytes
In principle, the reticulocyte count is a mechanistic test. It localizes anemia to a production problem or a survival problem before any disease is named. In practice, clinicians often experience it differently. Many interpret the reticulocyte count as a diagnostic clue rather than a physiologic localization tool. The distinction is subtle but important. The test is mechanistic. The user may experience it as diagnostic.
Clinical habits also vary. Hematologists typically check reticulocytes early, while many primary care clinicians move directly to morphology. These differences often reflect training patterns rather than biologic differences. The physiology does not change. Only the entry point does.
What differs between clinicians is not understanding of physiology but which physiologic question they ask first.
Localizing the failure
Once anemia is identified as a production problem, localization is not complete. The next task is not to list diagnoses. It is to determine which component of erythropoiesis is failing. Production can falter because:
- required materials are missing
- stimulation is insufficient
- the marrow machinery is defective
- the marrow environment is occupied
These are not diagnoses. They are failure modes. Each one narrows the diagnostic field and directs testing along a different path.
Mechanistic categories do not compete with diseases. They organize them physiologically.
Where morphology belongs
Cell size and other morphologic features are valuable, but their role is often misunderstood. Morphology is not a primary branch point in physiologic reasoning. It does not localize failure. It modifies probability.
Mean corpuscular volume is frequently the first abnormal value clinicians notice, and it can immediately suggest a pattern of disturbed erythropoiesis. But seeing a pattern is not the same as localizing a failure. Morphology is an observational clue, not a localization step.
Put simply:
Pattern may guide attention. Mechanism must guide reasoning.
Size suggests patterns. Physiology identifies failures. Diagnosis names diseases.
Those are different cognitive operations.
What different tests actually do
Not all tests play the same cognitive role. Diagnostic studies contribute at different stages of clinical reasoning:
| Test | Role in clinical reasoning | What it tells you |
|---|---|---|
| MCV | Pattern detector | Suggests which physiologic processes may be disturbed |
| Reticulocyte count | Physiologic branch point | Production vs loss/destruction |
| Ferritin | Mechanism probe | Whether substrate supply is adequate |
| Erythropoietin | Signal probe | Whether regulatory stimulation is intact |
| Bone marrow biopsy | Mechanism confirmer | Whether the factory itself is defective |
| JAK2 mutation | Disease identifier | Names a specific disorder |
Seen this way, tests do not simply diagnose disease. They progressively constrain physiology. Some tests localize failure. Some explain it. A few name it outright. Each result shrinks the map of possible failures.
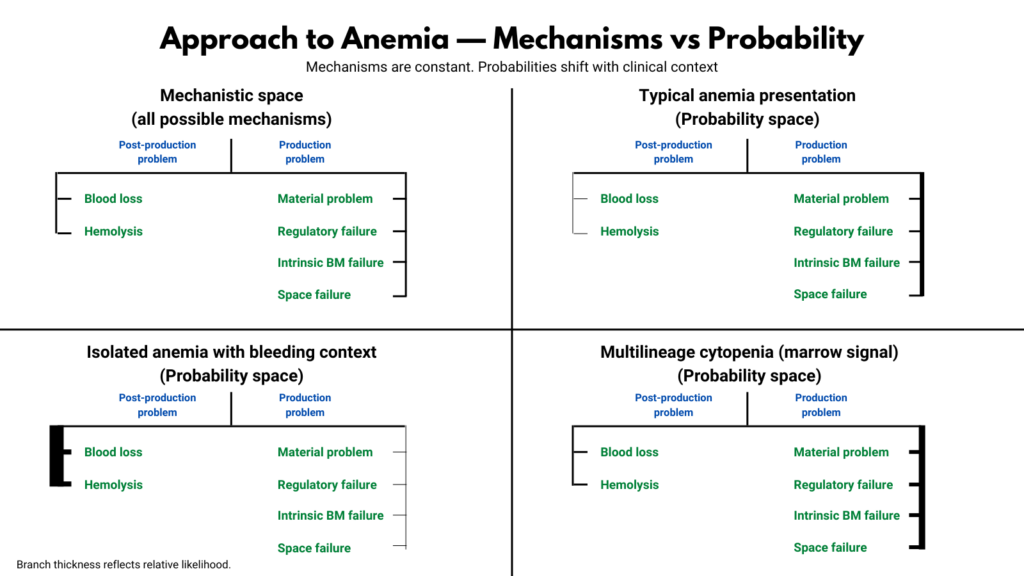
Possibility versus probability
Mechanistic frameworks describe what is biologically possible. Clinical reasoning must also account for what is statistically likely. These are not the same map.
A physiologic diagram is a possibility map. It shows every mechanism that can produce anemia. But when a clinician evaluates a real patient, probability immediately reshapes that landscape. Age, comorbidities, medications, tempo, and context all alter which regions of that map matter.
Diagnostic error arises when possibility maps are mistaken for probability maps.
The purpose of a mechanistic framework is not to rank diagnoses. It is to ensure none are forgotten.
Mechanism as a rescue tool
It is entirely possible to manage many patients successfully using pattern recognition alone. But mechanistic reasoning serves purposes that pattern recognition cannot:
- it explains why patterns occur
- it unifies diverse diseases under common principles
- it clarifies atypical presentations
- it prevents premature closure
- it allows reasoning when findings conflict
Pattern recognition manages the common. Mechanism rescues the uncommon. Neither replaces the other; each protects against the other’s blind spots.
For this reason, mechanistic reasoning is not always the fastest strategy. But it is the most reliable when cases become complex.
A case where mechanism rescues pattern
Consider a patient referred for evaluation of anemia with a normal MCV. Pattern recognition points toward the familiar differential of normocytic anemia: inflammation, kidney disease, endocrine dysfunction, or marrow disorders. A standard morphologic approach might begin ordering tests across that list.
But the reticulocyte count is elevated.
That single physiologic observation immediately changes the terrain. The marrow is not failing. It is responding. The problem is not production. It is loss.
Within seconds, the diagnostic universe collapses from dozens of possibilities to two physiologic categories: bleeding or hemolysis.
Further testing confirms hemolysis. The final diagnosis is autoimmune hemolytic anemia.
Nothing about the initial morphology suggested that diagnosis. The MCV was normal. The indices were unremarkable. Pattern alone would not have pointed there. Mechanism did. In practice, the answer is not always this immediate or this clean. But even when mechanism does not yield a single diagnosis, it still sharply narrows the field.
This is the practical value of physiologic reasoning. It does not replace pattern recognition. It rescues it when pattern becomes ambiguous.
A practical synthesis
In real clinical practice, pattern recognition often starts the evaluation of anemia. Mechanistic reasoning ensures that it stays on course. One is efficient. The other is stabilizing. Together they form a complete diagnostic strategy.
Pattern begins.
Mechanism directs.
Diagnosis concludes.
A final principle
Good clinicians do not begin by naming diseases. They begin by locating failures. Ordering tests is therefore not mere data gathering. It is physiologic interrogation.1
Anemia is no exception.
Synthesis: how to actually practice with this model
- Let pattern start the evaluation because it is fast and aligns with how labs present.
- Use reticulocytes deliberately as the first physiologic branching step, especially when indices are normocytic, mixed, or discordant with the clinical story.
- Within production failure, move explicitly through materials–signal–machinery–space using targeted tests that localize mechanism and, when possible, bridge to diagnosis.
- Switch from pattern to physiology the moment the pattern fails to fully explain the anemia.
- Remember that good clinicians begin by locating failures, not naming diseases; diagnosis is the terminus of a structured localization process, not its substitute.