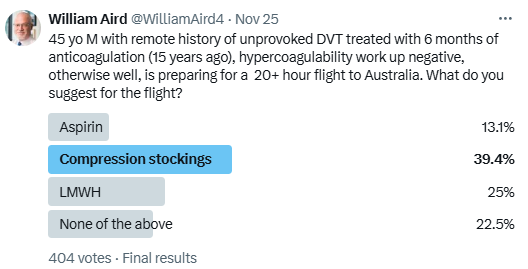
I posted a poll on Twitter asking the following:
Bottom Line
- Long-distance air travel, typically defined as long-distance air travel lasting > 4 hours (though some define it as > 8 hours), increases the risk of VTE 2- to 4-fold.
- The association between air travel and VTE is strongest for flights > 8 to 10 h and is increased in the presence of VTE risk factors such as recent surgery.
- Prevention strategies include calf muscle exercises, frequent ambulation, and aisle seating when possible, compression stockings, aspirin and LMWH.
- There is scant evidence to inform decisions about prevention. Clinical practice guidelines recommend the following:
| Guideline | Not at increased risk for thrombosis | At increased risk for thrombosis |
|---|---|---|
| American College of Chest Physicians (ACCP) Guidelines | For long-distance travelers not at increased risk of VTE, use of GCS is not recommended. | For long-distance travelers (>6 hours travel) at increased risk of VTE, the ACCP recommends frequent ambulation, calf muscle exercise, sitting in an aisle seat if feasible, and use of properly fitted below-the-knee graduated compression stockings (GCS) providing 15–30 mmHg of pressure at the ankle during travel. |
| American Society of Hematology Guidelines | For travelers without risk factors, ASH suggests not using GCS, LMWH, or aspirin for VTE prophylaxis. | For long-distance travelers (>4 hours travel) at substantially increased VTE risk (e.g., recent surgery, prior history of VTE, postpartum, active malignancy, or ≥2 risk factors, including combinations of the above with hormone replacement therapy, obesity, or pregnancy) the ASH guideline panel suggests GCS or prophylactic low molecular weight heparin (LMWH). If GCS or LMWH are not feasible, ASH suggests using aspirin rather than no VTE prophylaxis. |
| British Society of Hematology Guidelines | There is indirect evidence that maintaining mobility may prevent VTE and, in view of the likely pathogenesis of travel-related VTE, maintaining mobility is a reasonable precaution for all travelers on journeys over 3 h. Global use of compression stockings and anticoagulants for long distance travel is not indicate. | Travelers at the highest risk of travel-related thrombosis undertaking journeys of >3 h should wear well fitted below knee compression hosiery. Where pharmacological prophylaxis is considered appropriate, anticoagulants as opposed to anti-platelet drugs are recommended, based on the observation that in other clinical scenarios they provide more effective thrombo-prophylaxis. |
Introduction
- Long-distance air travel, typically defined as long-distance air travel lasting > 4 hours (though some define it as > 8 hours), increases the risk of VTE 2- to 4-fold.
- The absolute risk of a travel-related VTE is small and of little concern to the average traveler.
- Flight-related thrombosis tends to attract much more media attention compered to other risk factors for thrombosis, such as having a cast or undergoing orthopedic surgery.1
- The association between air travel and VTE is strongest for flights > 8 to 10 h and is increased in the presence of VTE risk factors such as recent surgery.
- “Concerns about travel-related VTE are so prevalent that the American Society of Hematology (ASH) chose to include recommendations for long-distance travelers in its guidelines for VTE prophylaxis in hospitalized and non-hospitalized medical patients, which were released in late 2018.”2
- The risk for thrombosis not limited to air travel. It has also been reported with overland travel (travel by car, bus, or train).3
- Prevention strategies include calf muscle exercises, frequent ambulation, and aisle seating when possible, compression stockings, aspirin and LMWH.
Definition
- The definition of long-distance air travel as lasting anywhere from >3 hours to >10 hours. Although no standard definition exists, >4 hours is most often used.4
- Post-flight observation period ranges from “hours after landing” to ≥8 weeks; 4 weeks, however, is most common. For example, British Society of Hematology guideline states that: “VTE may be attributable to travel if it occurs up to 8 weeks following the journey.”
- Study outcomes range from asymptomatic DVT to symptomatic DVT/PE to severe or fatal PE.
History
- John Homans is widely reported to have published the first description of venous thromboembolism (VTE) in relation to long-distance travel in 1954; he wrote that prolonged dependency stasis related to the sitting position may result in deep vein thrombosis (DVT).5
- However, according to Czuprynska and Arya, four cases of phlebitis due to air travel were described three years earlier in the French literature.6
Epidemiology
- Existing studies are heterogeneous in design, which prevents meaningful comparisons and robust conclusions.
- VTE, including both deep vein thrombosis (DVT) and PE, occurs in approximately one per 1,000 adults per year in the general population. Prolonged travel (flights of four hours or longer) is associated with a 2-4-fold increase in risk, with an absolute risk of an event within four weeks of the flight of about one in 4,600 flights. This risk could increase in people with other predisposing factors for thrombosis/7
- Centers for Disease Control and Prevention (CDC):
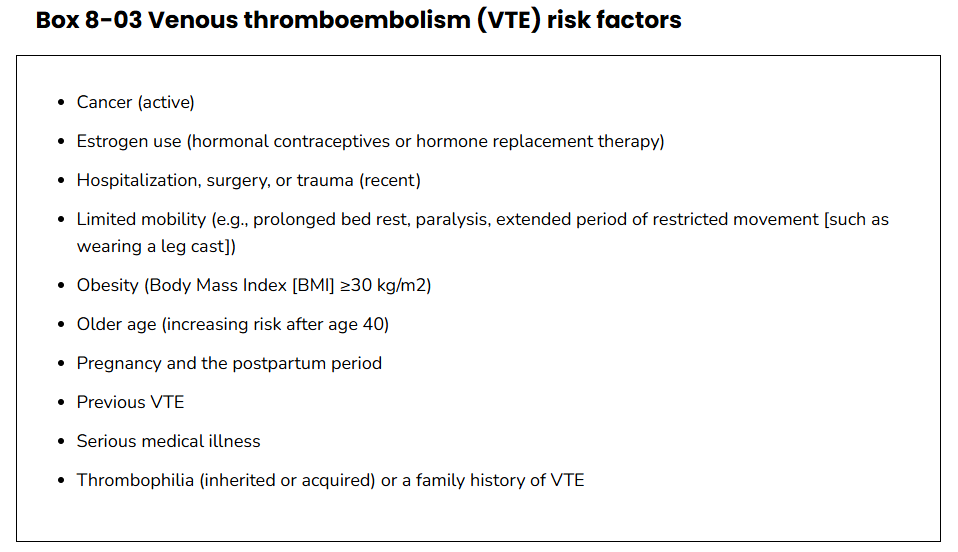
- The annual incidence of VTE in the general population is estimated to be 0.1% but is greater in subpopulations with risk factors for VTE (Box 8-03, see below). The actual incidence of travel-related VTE is difficult to determine because there is no national surveillance for VTE and no consensus on the definition of travel-related VTE, particularly regarding duration of travel and period of observation after travel.
- In general, the incidence of air travel–related VTE appears to be low. For flights >4 hours, one study reported an absolute risk for VTE of 1 in 4,656 flights; another reported an absolute risk of 1 in 6,000 flights.8
- People who travel on long-distance flights generally are healthier and therefore at a lower risk for VTE than the general population.
- Five prospective studies conducted to assess the incidence of DVT after travel >8 hours among travelers at low to intermediate risk for VTE yielded an overall VTE incidence of 0.5%; the incidence of symptomatic VTE was 0.3%.
- Studies indicate that long-distance air travel might increase a person’s overall risk for VTE by 2- to 4-fold.
- Some studies found that long-distance air travel increased the risk of VTE occurring, while others either found no definitive evidence of increased risk, or found that risk increased only if ≥1 additional VTE risk factors were present.
- Level of risk correlates with duration of travel and with preexisting risk factors for VTE. Risk decreases with time after air travel and returns to baseline by 8 weeks; most air travel–related VTE occurs within the first 1–2 weeks after the flight.
- Some studies have shown that 75%–99.5% of people who developed travel-related VTE had ≥1 preexisting risk factor; one study showed that 20% had ≥5 risk factors. For travelers without preexisting risk factors, the risk of travel-related VTE is low.
- British Society of Hematology Guidelines on travel-related venous thrombosis, 2011:
- Long duration travel is a weak risk factor for the development of VTE.
- The incidence of VTE in low and intermediate risk flyers after flights of:
- > 4 h is 1 in 4656
- > 8 h is about 0.5%
- Severe symptomatic PE in the period immediately after travel is extremely rare after flights of <8 h. In flights over 12 h the rate is 5 per million.
- The risk of travel-related thrombosis is higher in individuals with pre-existing risk factors for the development of VTE.
- VTE may be attributable to travel if it occurs up to8 weeks following the journey.
Mechanisms
- Risk factors for travel-related VTE include:
- Air cabin risk factors:
- Hypobaric hypoxia from air pressure changes in the cabin (may trigger a coagulation cascade, the body’s natural clotting response).
- Patient risk factors:9
- Most individuals with travel-associated VTE have one or more known risk factors for thrombosis.10
- Risk factors include:
- Age
- Active cancer diagnosis
- Pregnancy
- Oral contraceptive use
- Recent surgery
- Obesity
- Hereditary conditions In its recommendations for travel-associated VTE, the ASH guideline panel considered patients with these factors at greater risk for travel-related VTE, but the panel noted that little evidence exists showing that patients with prior VTE or those with total joint arthroplasty were at any increased risk for travel-related VTE ASH letter
- Especially tall or short passengers may have an increased risk.11
- Air cabin risk factors:
- Virchow’s classic triad for thrombus formation is:
- Venous stasis:1213
- Prolonged, cramped sitting during long-distance travel interferes with venous flow in the legs, creating venous stasis.
- Cramped position where the seat may press against the popliteal vein behind the knee, a common site of clots (Seat-edge pressure to the popliteal area of the legs can aggravate venous stasis and contribute to vessel wall damage.)
- Travelers’ ability to move around the cabin might be hampered by flight conditions such as turbulence, their location on the plane, or flight attendants’ use of the aisles.
- Vessel wall damage (including endothelial cell dysfunction)
- Hypercoagulable state:
- Several studies investigated the effect of prolonged immobilization on thrombin generation, but conflicting results were shown.
- Venous stasis:1213
- Studies of the pathophysiologic mechanisms for the increased risk of VTE after long-distance travel have not produced consistent results, but venous stasis appears to play a major role. Other factors specific to air travel might increase coagulation activation, particularly in travelers with preexisting risk factors for VTE.14
- Dehydration may also play a role in risk for VTE.1517
- GCS appear to reduce asymptomatic DVT in travelers and are generally well tolerated
- ACCP guidance:
- Stockings come in different sizes.
- If a stocking is too tight around the knee it can prevent essential venous return, causing the blood to pool around the knee.
- Compression stockings should be fitted properly.
- A stocking that is too tight could cut into the skin on a long flight and potentially cause ulceration and increased risk of DVT.
- Some stockings can be slightly thicker than normal leg covering and can be potentially restrictive with tight footwear.
- It is a good idea to wear stockings around the house prior to travel to ensure a good, comfortable fitting.
- Stockings were put on 2 to 3 h before the flight in most of the trials.
- The availability and cost of stockings can vary.
- Pharmacologic prophylaxis:18
- Decisions regarding use of pharmacologic prophylaxis for long-distance travelers at high risk should be made on an individual basis.
- When the potential benefits of pharmacologic prophylaxis outweigh the possible adverse effects, anticoagulants rather than antiplatelet drugs (e.g., aspirin) are recommended
- Hydration:19
- No evidence exists for an association between dehydration and travel-related VTE. Furthermore, no direct evidence exists to support the concept that drinking plenty of nonalcoholic beverages to ensure adequate hydration or avoiding alcoholic beverages has a protective effect. Therefore, maintaining hydration is reasonable and unlikely to cause harm, but it cannot be recommended specifically to prevent travel-related VTE.
- In-flight mobility & seat assignment:20
- Immobility while flying is a risk for VTE. Indirect evidence suggests that maintaining mobility could prevent VTE. In view of the role that venous stasis plays in the pathogenesis of travel-related VTE, recommending frequent ambulation and calf muscle exercises for long-distance travelers is reasonable.
- An aisle seat also might be a protective factor to reduce the risk of developing VTE. In one study, travelers seated in window seats experienced a 2-fold increase in general risk for VTE compared with passengers in aisle seats; travelers with a body mass index ≥30 kg/m2 who sat in window seats had a 6-fold increase in risk. Conversely, aisle seats are reported to have a protective effect compared with window or middle seats, probably because travelers are freer to move around.
- Representative Studies
- Scurr et al, 2001:
- Methods:
- 89 male and 142 female passengers over 50 years of age with no history of VTE.
- Passengers were randomly allocated to one of two groups:
- One group wore class-I below-knee graduated elastic compression stockings
- The other group did not
- All the passengers made journeys lasting more than 8 h per flight (median total duration 24 h), returning to the UK within 6 weeks.
- Duplex ultrasonography was used to assess the deep veins before and after travel. Blood samples were analyzed for two specific common gene mutations, factor V Leiden (FVL) and prothrombin G20210A (PGM), which predispose to venous thromboembolism.
- Results:
- Deep vein thrombosis (DVT):
- 12/116 passengers (10%; 95% CI 4·8–16·0%) developed symptomless DVT in the calf (five men, seven women).
- None of these passengers wore elastic compression stockings, and two were heterozygous for FVL.
- None of the passengers who wore class-I compression stockings developed DVT (95% CI 0–3·2%)
- Superficial thrombophlebitis:
- Four further patients who wore elastic compression stockings, had varicose veins and developed superficial thrombophlebitis.
- One of these passengers was heterozygous for both FVL and PGM.
- Deep vein thrombosis (DVT):
- Conclusions:
- We conclude that:
- Symptomless DVT might occur in up to 10% of long-haul airline travelers.
- Wearing of elastic compression stockings during long-haul air travel is associated with a reduction in symptomless DVT.
- We conclude that:
- Methods:
- Cesarone et al. 2002 (LONFLIT3 study):
- 300 subjects at high risk for DVT were randomized, after informed consent, into three groups:
- A control group that had no prophylaxis
- An aspirin treatment group, in which patients were treated with 400 mg (tablets of oral, soluble aspirin; one dose daily for 3 days, starting 12 hours before the beginning of the flight)
- A low-molecular-weight heparin (LMWH) group, in which one dose of enoxaparin was injected between 2 and 4 hours before the flight. The dose was weight-adjusted (1,000 IU [equivalent to 0.1 mL per 10 kg of body weight).
- Of the 100 included subjects in each group, a total of 249 subjects completed the study (dropouts due to low compliance or traveling/connections problems were 17%).
- Of the 82 subjects in the control group, there were 4.82% of subjects with DVT with two superficial thromboses. In total 4.8% of limbs suffered a thrombotic event.
- Of 84 subjects in the aspirin treatment group, there were 3.6% of patients with DVT and three superficial thrombosis. In total 3.6% of limbs had a thrombotic event.
- In the LMWH group (82 subjects), there were no cases of DVT. One superficial thrombosis was documented. In total only 0.6% of limbs had a thrombotic event (p<0.002 in comparison with the other two groups).
- DVT was asymptomatic in 60% of subjects.
- 85% of DVTs were observed in passengers in non-aisle seats.
- Conclusions: One dose of LMWH is an important option to consider in high-risk subjects during long-haul flights.
- 300 subjects at high risk for DVT were randomized, after informed consent, into three groups:
- Schwartz et al, 2003:
- Methods:
- 964 passengers returning from long-haul flights (flight duration, > or =8 hours) and 1213 nontraveling control subjects.
- Excluded were participants who were being treated with anticoagulant drugs or who used compression stockings.
- Main outcome measures were the incidence of ultrasonographically diagnosed thrombosis in the calf muscle and deep veins, symptomatic pulmonary embolism, and death.
- Results:
- VTE in 27 passengers (2.8%) and 12 controls (1.0%) (risk ratio [RR], 2.83; 95% confidence interval [CI], 1.46-5.49).
- 20 passengers (2.1%) and 10 controls (0.8%) presented with isolated calf muscle venous thrombosis (RR, 2.52; 95% CI, 1.20-5.26).
- 7 passengers (0.7%) and 2 controls (0.2%) presented with deep venous thrombosis (RR, 4.40; 95% CI, 1.04-18.62).
- Symptomatic pulmonary embolism was diagnosed in 1 passenger with deep venous thrombosis (P =.44).
- Only 3 out of 964 travelers had symptomatic VTE, which would give an incidence of 0.3%.
- In the control group, 1 had a symptomatic DVT (giving an incidence of 0.08%) and this was a recurrent proximal event
- 13 (48%) of the 27 patients who were diagnosed with VTE had a past history of VTE.
- All of these individuals had normal findings at baseline ultrasonography.
- Passengers with isolated calf muscle venous thrombosis or deep venous thrombosis had at least 1 risk factor for venous thrombosis (>45 years of age or elevated body mass index in 21 of 27 passengers).
- The follow-up after 4 weeks revealed no further venous thromboembolic event.
- Conclusions:
- Long-haul flights of 8 hours and longer double the risk for isolated calf muscle venous thrombosis. This translates into an increased risk for deep venous thrombosis as well. In our study, flight-associated thrombosis occurred exclusively in passengers with well-established risk factors for venous thrombosis.
- Methods:
- Kuipers et al, 2007:
- Cohort study among employees of large international companies and organizations.
- The occurrence of symptomatic venous thrombosis was linked to exposure to air travel, as assessed by travel records provided by the companies and organizations.
- A long-haul flight was defined as a flight of at least 4 h and participants were considered exposed for a post-flight period of 8 wk.
- 8,755 employees were followed during a total follow-up time of 38,910 person-years (PY).
- The total time employees were exposed to a long-haul flight was 6,872 PY.
- In the follow-up period, 53 thromboses occurred, 22 of which occurred within 8 wk of a long-haul flight, yielding an incidence rate of 3.2/1,000 PY, as compared to 1.0/1,000 PY in individuals not exposed to air travel (incidence rate ratio 3.2, 95% confidence interval 1.8-5.6).
- This rate was equivalent to a risk of one event per 4,656 long-haul flights.
- The risk increased with exposure to more flights within a short time frame and with increasing duration of flights.
- The incidence was highest in the first 2 wk after travel and gradually decreased to baseline after 8 wk.
- The risk was particularly high in employees under age 30 y, women who used oral contraceptives, and individuals who were particularly short, tall, or overweight.
- Conclusions: The risk of symptomatic venous thrombosis after air travel is moderately increased on average, and rises with increasing exposure and in high-risk groups.
- Scurr et al, 2001:
- Systematic reviews:
- Philbrick et al, 2007:
- Twenty-four published reports, totaling 25 studies, met inclusion criteria (6 case control studies, 10 cohort studies, and 9 randomized controlled trials).
- Significantly related to VTE rate:
- Method of screening for VTE [screening ultrasound compared to usual clinical care
- Outcome measure [all VTE compared to pulmonary embolism (PE) only]
- Duration of travel (<6 hours compared to 6–8 hours)
- Clinical risk (“higher” risk travelers compared to “lower”)
- Clinical VTE after prolonged travel is rare [27 PE per million flights diagnosed through usual clinical care, 0.05% symptomatic deep venous thrombosis (DVT) diagnosed through screening ultrasounds]
- Asymptomatic thrombi of uncertain clinical significance are more common.
- Graduated compression stockings prevented travel-related VTE (P<0.05 in 4 of 6 studies), aspirin did not, and low-molecular-weight heparin (LMWH) showed a trend toward efficacy in one study.
- Conclusions:
- All travelers, regardless of VTE risk, should avoid dehydration and frequently exercise leg muscles.
- Travelers on a flight of less than 6 hours and those with no known risk factors for VTE, regardless of the duration of the flight, do not need DVT prophylaxis.
- Travelers with 1 or more risk factors for VTE should consider graduated compression stockings and/or LMWH for flights longer than 6 hours.
- Kuipers et al. 2007:
- Case-control studies:
- 10 publications in which travel frequency of cases with symptomatic VT was compared with a control population without VT.
- The pooled odds ratio of all studies together was 1.7. After exclusion of the four studies with a potential bias, this increased to 2.3.
- Six studies contained data on air travel only or separately for air travel and other modes of travel. The pooled odds ratio for air travel of any duration of all studies was 1.4 (95% CI 0.9–2.0). After exclusion of three studies with a potential bias, the pooled odds ratio of the remaining studies was 1.9.
- Three publications showed data on long-distance air travel, defined as flights longer than 8 h, with odds ratios ranging from 1.3 to 7.9 and a pooled odds ratio of 1.9. After exclusion of one study with a potential bias [15], this pooled odds ratio increased to 3.9 (95% CI 1.4–10.7).
- Randomized controlled trials:
- A total of 11 randomized trials were conducted to assess the effect of various prophylactic measures on the risk of VT after air travel.
- a number of air travelers, varying from 148 to 833, making long-haul flights (>7 h) were randomized to either a control group or an intervention group that received elastic compression stockings, aspirin, heparin, venoruton (hydroxyethylrutosides), pycnogenol (pine tree extract containing procyanidins, bioflavonoids and organic acids) or FLITE tabs (containing pycnogenol and nattokinase, a soybean extract).
- All passengers were routinely screened for VT by ultrasound after their flight (within a maximum of 48 h).
- All but one of these studies was conducted by the same research group.
- Majority of the thrombotic events in all trials were asymptomatic.
- Credibility of these trials questioned We therefore will not discuss the results of these trials in this systematic review.
- In the only remaining trial, the effect of elastic compression stockings was assessed in 231 airline passengers travelling at least 8 h. None of the 100 passengers who were randomized to the elastic compression stockings group developed VT, whereas 12 of the 100 control passengers did, yielding a relative risk of 0.04 (95% CI 0–0.6). However, four passengers wearing elastic compression stockings developed superficial thrombophlebitis, whereas none of the control passengers did.
- Conclusions: We conclude that:
- Long-distance travel increases the risk of VT approximately two to fourfold.
- The absolute risk of a symptomatic event within 4 weeks of flights longer than 4 h is 1 ⁄ 4600 flights.
- The risk of severe pulmonary embolism (PE) occurring immediately after air travel increases with duration of travel, up to 4.8 per million in flights longer than 12 h.
- The mechanism responsible for the increased risk of VT after (air) travel has insufficiently been studied to draw solid conclusions, but one controlled-study showed evidence for an additional mechanism to immobilization that could lead to coagulation activation after air travel.
- Chandra et al, 2009
- Of 1560 identified abstracts, 14 studies (11 case-control, 2 cohort, and 1 case-crossover) met inclusion criteria, including 4055 cases of VTE.
- Compared with nontravelers, the overall pooled relative risk for VTE in travelers was 2.0 (95% CI, 1.5 to 2.7).
- Significant heterogeneity was present because of the method for selecting control participants (P = 0.008): whether the studies used control participants who had been referred for VTE evaluation or non-referred control participants.
- When the studies that used referred control participants were excluded, the pooled relative risk for VTE in travelers was 2.8 (CI, 2.2 to 3.7), without significant heterogeneity.
- A dose-response relationship was identified, with an 18% higher risk for VTE for each 2-hour increase in duration of travel by any mode (P = 0.010) and a 26% higher risk for every 2 hours of air travel (P = 0.005).
- Conclusions: Travel is associated with a nearly 3-fold higher risk for VTE, with a dose-response relationship of 18% higher risk for each 2-hour increase in travel duration. Heterogeneity in results of previous studies was due to selection bias toward the null from use of referred control participants.
- Clarke et al, Cochrane Review, 2021:
- Randomized trials of compression stockings versus no stockings in passengers on flights lasting at least four hours. Trials in which passengers wore a stocking on one leg but not the other, or those comparing stockings and another intervention were also eligible.
- Eleven randomized trials (n = 2906) were included in this review:
- Nine (n = 2821) compared wearing graduated compression stockings on both legs versus not wearing them
- One trial (n = 50) compared wearing graduated compression tights versus not wearing them
- One trial (n = 35) compared wearing a graduated compression stocking on one leg for the outbound flight and on the other leg on the return flight.
- Eight trials included people judged to be at low or medium risk of developing DVT (n = 1598) and two included high-risk participants (n = 1273).
- All flights had a duration of more than five hours.
- Fifty of 2637 participants with follow-up data available in the trials of wearing compression stockings on both legs had a symptomless DVT:
- Three wore stockings
- 47 did not (odds ratio (OR) 0.10, 95% confidence interval (CI) 0.04 to 0.25, P < 0.001; high-quality evidence).
- There were no symptomless DVTs in three trials.
- Sixteen of 1804 people developed superficial vein thrombosis, four wore stockings, 12 did not (OR 0.45, 95% CI 0.18 to 1.13, P = 0.09; moderate-quality evidence).
- No deaths, pulmonary emboli or symptomatic DVTs were reported.
- Wearing stockings had a significant impact in reducing edema (mean difference (MD) -4.72, 95% CI -4.91 to -4.52; based on six trials; low-quality evidence).
- A further two trials showed reduced edema in the stockings group but could not be included in the meta-analysis as they used different methods to measure edema. No significant adverse effects were reported.
- Conclusions: There is high-quality evidence that airline passengers similar to those in this review can expect a substantial reduction in the incidence of symptomless DVT and low-quality evidence that leg edema is reduced if they wear compression stockings (all the stockings in the nine trials included in this review were below-knee compression stockings). There is moderate-quality evidence that superficial vein thrombosis may be reduced if passengers wear compression stockings. We cannot assess the effect of wearing stockings on death, pulmonary embolism or symptomatic DVT because no such events occurred in these trials. Randomized trials to assess these outcomes would need to include a very large number of people.
- Case-control studies:
- Philbrick et al, 2007:
- Clinical guidelines:
- 2012 American College of Chest Physicians (ACCP) Guidelines:
- ACCP 2012 guidelines (Grade 2C: weak recommendations, low- or very low-quality evidence):
- For long-distance travelers (>6 hours travel) at increased risk of VTE, the ACCP recommends frequent ambulation, calf muscle exercise, sitting in an aisle seat if feasible, and use of properly fitted below-the-knee graduated compression stockings (GCS) providing 15–30 mmHg of pressure at the ankle during travel.
- For long-distance travelers not at increased risk of VTE, use of GCS is not recommended.
- ACCP suggests against the use of aspirin or anticoagulants to prevent VTE in long-distance travelers.
- ACCP 2012 guidelines (Grade 2C: weak recommendations, low- or very low-quality evidence):
- 2018 American Society of Hematology Guidelines:
- ASH 2018 guidelines (conditional recommendations, very low certainty in the evidence of effects):
- For long-distance travelers (>4 hours travel) at substantially increased VTE risk (e.g., recent surgery, prior history of VTE, postpartum, active malignancy, or ≥2 risk factors, including combinations of the above with hormone replacement therapy, obesity, or pregnancy) the ASH guideline panel suggests GCS or prophylactic low molecular weight heparin (LMWH).
- If GCS or LMWH are not feasible, ASH suggests using aspirin rather than no VTE prophylaxis.
- For travelers without risk factors, ASH suggests not using GCS, LMWH, or aspirin for VTE prophylaxis.
- ASH 2018 guidelines (conditional recommendations, very low certainty in the evidence of effects):
- 2011 British Society of Hematology Guidelines:
- There is no evidence for an association between dehydration and travel-associated VTE and so whilst maintaining good hydration is unlikely to be harmful, it cannot be strongly recommended for prevention of thrombosis.
- There is indirect evidence that maintaining mobility may prevent VTE and, in view of the likely pathogenesis of travel-related VTE, maintaining mobility is a reasonable precaution for all travelers on journeys over 3 h.
- Global use of compression stockings and anticoagulants for long distance travel is not indicated.
- Assessment of risk should be made on an individual basis but it is likely that recent major surgery (within 1 month), active malignancy, previous unprovoked VTE, previous travel-related VTE with no associated temporary risk factor or presence of more than one risk factor identifies those travelers at highest thrombosis risk.
- Travelers at the highest risk of travel-related thrombosis undertaking journeys of >3 h should wear well fitted below knee compression hosiery.
- Where pharmacological prophylaxis is considered appropriate, anticoagulants as opposed to anti-platelet drugs are recommended, based on the observation that in other clinical scenarios they provide more effective thrombo-prophylaxis.
- Center for Disease Control (CDC):
- General protective measures for long-distance travelers include calf muscle exercises, frequent ambulation, and aisle seating when possible. Additional protective measures for long-distance travelers at increased risk of VTE include properly fitted below-the-knee GCS and anticoagulant prophylaxis, but only in particularly high-risk cases where the potential benefits outweigh the risks.
- 2012 American College of Chest Physicians (ACCP) Guidelines:
- Expert opinion from ASH Clinical News article on Planes, Trains, and VTEs
- This paper offers an excellent perspective on long haul flight associated VTE. Included in the discussion are two underexplored areas:
- Use of DOACs:
- “It is reasonable to use a DOAC for prevention or as a prophylactic dose instead of LMWH,” she [Dr. Susan Kahn] said, noting that these oral medications are rapid-acting and do not require injection. “However, we have no studies that have looked at that [option], so we did not include them in [ASH’s] recommendations.
- One review article looked at the possible role of DOACs in treatment of travel-related VTE, concluding that DOACs could be used “to treat travel-related VTE, as there is no evidence suggesting that it is different from VTE in general,” with the exception of patients with active malignancy, where LMWH is preferred.21
- “In my personal practice, if I think prophylaxis is warranted, I tell a patient to take the tablets,” Dr. [Mark] Crowther said, noting that the literature on the use of prophylactic DOACs for travel-related VTE is nonexistent.
- Dr. [Marc] Carrier agreed, saying he has seen increasing use of DOACs instead of injectable LMWH. “It’s all about risks and benefits. I would estimate the benefit from peace of mind and reassurance against the risk of bleeding from one tablet is very small.”
- The Provoked vs. Unprovoked Debate:
- In the rare case when travel-related VTE occurs or is suspected, questions build. Clinicians must decide whether the clot was provoked by travel or some other factor.
- “This is a controversial but important topic,” Dr. [Marc] Carrier explained, “because this decision will make a difference in whether a patient is bound to long-term anticoagulation or can stop anticoagulation after three months. Clinicians have to make a judgment call.”
- “Air travel is not like a recent fracture, where risk is clear,” he [Dr. Mark Crowther] said. “Air travel–related VTE generally is considered provoked, but in the setting of a weak risk factor.”
- Dr. Kahn agreed. “To say that air travel represents a provoked episode of VTE doesn’t seem to be that logical to those who work in the field, but neither does calling it unprovoked. Travel-related VTE falls in that gray zone we call ˜weakly provoked.”
- If the decision is made to stop anticoagulation after three months, one thing we would usually do in a patient with travel-related thrombosis is to offer prophylaxis to prevent another episode during future travel.
- With so many differing opinions about how much air travel contributes to VTE risk, however, definitive recommendations about preventing travel-related VTE are still up in the air.