The Question
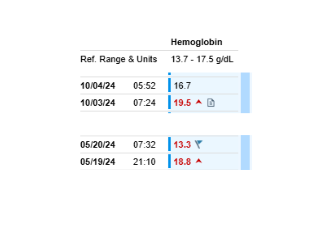
A patient repeatedly presents to the hospital with an elevated hemoglobin that then falls precipitously by the following day.
Shown here are two of several similar admissions in the same patient. In one episode, the hemoglobin fell from 18.8 g/dL on arrival to 13.3 g/dL nine hours later.
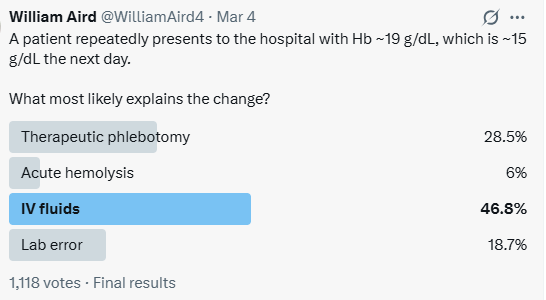
What is the most likely explanation?
- Therapeutic phlebotomy
- Acute hemolysis
- IV fluids
- Laboratory artifact
Poll Results
We posed this question on Twitter.
The majority answer was IV fluids, which is correct.
At first glance, such a large change in hemoglobin may seem surprising. But the explanation is not a matter of intuition or clinical experience. It follows directly from basic physiology and a simple quantitative calculation.
Working Through the Calculation
Assumptions
For the calculations below we assume:
- Initial hemoglobin: 18.8 g/dL
- Blood volume when euvolemic: ≈5 L
- Severe dehydration contracts blood volume to ≈4 L (~20% contraction)
- Normal saline: ~25% remains intravascular
- Therapeutic phlebotomy: ~0.5 L whole blood per unit
- RBC mass remains constant unless blood is removed or destroyed
Simple Calculation Method
Convert hemoglobin to g/L for consistency with blood volume.
19 g/dL ≈ 190 g/L
Initial RBC mass proxy:Hb × BV=190 ×5 = 950
After phlebotomy of x L
- RBC mass decreases by 190 × x
- blood volume decreases by x
After normal saline of y L
- blood volume increases by 0.25 × y
- RBC mass unchanged
Worked calculations
Scenario 1
Patient has one-unit phlebotomy and receives 1 L normal saline
Hb 19 g/dL = 190 g/L
Total Hb (RBC mass proxy) = 190 g/L x 5 L = 950 g
1 unit phlebotomy removes 0.5 L whole blood = 95 g of Hb
New total Hb = 950 – 95 g = 855 g
New blood volume = 5 L – 0.5 L = 4.5 L
Receives 1 L normal saline – 0.25 L remains in IV space
New blood volume = 4.5 + 0.25 L = 4.75 L
Hb concentration = 855 g/4.75 L = 180 g/L or 18.0 g/dL
Scenario 2
Patient has 20% volume contraction and receives 4 L of normal saline
Hb 19 g/dL = 190 g/L
20% volume contraction reduces blood volume from 5 L –> 4L
Total Hb (RBC mass proxy) = 190 g/L x 4 L = 760 g
Receives 4 L normal saline – 1 L remains in IV space
New blood volume = 4 L + 1 L = 5 L
Hb concentration = 760 g/5 L = 152 g/L or 15.2 g/dL
The same approach can be applied to other scenarios. The table below summarizes the expected hemoglobin values under several common clinical conditions.
Summary of estimated hemoglobin values
| Scenario | Starting BV | Blood removed | NS given | Net intravascular change | Expected Hb |
|---|---|---|---|---|---|
| IV fluids only (euvolemic) | 5 L | 0 | 2 L | +0.5 L* | ~17.3 |
| IV fluids correcting dehydration** | 4 L | 0 | 4 L | +1.0 L | ~15.2 |
| Phlebotomy (1 unit) immediate*** | 5 L | 0.5 L | 0 | −0.5 L | ~18.8 |
| Phlebotomy after plasma refill**** | 5 L | 0.5 L | 0 | ~0 | ~16.9 |
| Phlebotomy + 1 L NS | 5 L | 0.5 L | 1 L | −0.25 L | ~18.0 |
* Normal saline: approximately 25% remains in the intravascular space, with the remainder distributing to the interstitial compartment.
** Dehydration scenario: starting blood volume of 4 L represents ~20% plasma volume contraction, consistent with severe dehydration.
*** Therapeutic phlebotomy removes whole blood, so both RBC mass and plasma volume decrease initially, resulting in little immediate change in hemoglobin concentration.
**** Plasma refill: over several hours after phlebotomy, interstitial fluid shifts into the intravascular space, restoring plasma volume while RBC mass remains reduced.
Evaluating the possible explanations
The calculations lead to the following conclusions.
| Mechanism | Physiologic change required | Approximate quantity |
|---|---|---|
| IV fluids (euvolemic) | ~40% plasma expansion | ~8 L saline |
| IV fluids correcting dehydration | Restoration of contracted plasma volume | ~2–4 L IV fluid |
| Therapeutic phlebotomy | Removal of ~30% RBC mass | ~1.4–1.6 L blood (~3 units) |
| Acute hemolysis | Destruction of ~30% RBC mass | Would cause severe illness |
| Laboratory artifact | No physiologic change | Possible but unlikely here |
Approximate quantities are derived from the calculations above and assume a euvolemic blood volume of ~5 L unless otherwise stated.
Why Phlebotomy Cannot Explain the Observation
Therapeutic phlebotomy removes whole blood, not just red cells.
This means both:
- RBC mass decreases
- plasma volume decreases
Because numerator and denominator fall together, hemoglobin concentration changes very little immediately after phlebotomy.
Even with plasma redistribution or IV fluids afterward, achieving a drop from 18.8 → 13.3 g/dL would require removing an implausibly large amount of blood and replacing that volume with plasma.
What About Hemolysis or Laboratory Error?
Hemolysis severe enough to reduce hemoglobin by ~30% within hours would typically produce clear clinical signs of acute illness.
Laboratory artifact is always possible, but in this case it was unlikely: the same pattern occurred during two separate hospital admissions.
The Clinical Context
This patient was a 60-year-old man with cyclical vomiting who repeatedly presented with:
- Hemoglobin ~19 g/dL on arrival
- Rapid fall to ~13 g/dL after rehydration
Severe dehydration produced hemoconcentration (high hemoglobin despite unchanged RBC mass), and IV fluids restored plasma volume, leading to rapid normalization of hemoglobin.
Take-Home Message
Rapid changes in hemoglobin concentration are rarely mysterious.
When red cell mass remains constant, hemoglobin simply reflects plasma volume.
With a few physiologic assumptions and a short calculation, the answer becomes clear.
Clinical reasoning grounded in quantitative physiology often beats intuition.