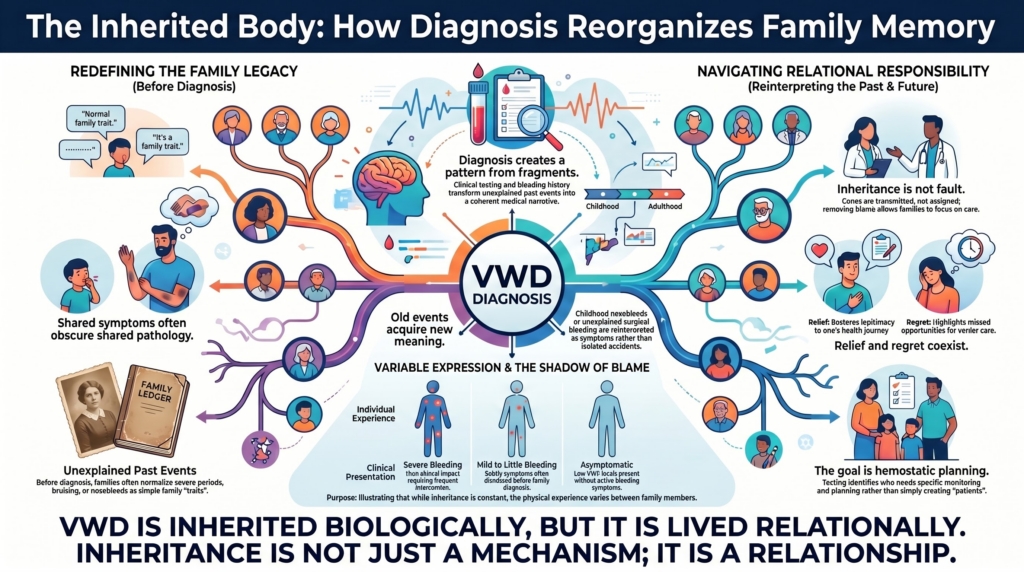
How diagnosis moves backward through time and outward through family
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
VWD is inherited.
That statement sounds simple. It is not. Inheritance is not only a genetic fact; it is a lived family experience.
When a child is diagnosed, the diagnosis does not stop with the child. It can reorganize family memory. A father remembers nosebleeds. A mother remembers heavy periods. A grandmother’s hysterectomy becomes relevant. An aunt’s postpartum hemorrhage is reinterpreted. A sibling asks whether they should be tested. A parent wonders whether they passed something on.
The family story changes. What once seemed ordinary becomes evidence. What once seemed private becomes shared. What once seemed bad luck becomes pattern.
Diagnosis moves backward through time and outward through family.
Family history is clinical evidence
Family history is central to VWD diagnosis. It can support inherited disease, identify relatives at risk, guide testing, and clarify whether bleeding is isolated or patterned. Diagnostic guidelines and reviews consistently emphasize the integration of bleeding phenotype, family history, and laboratory testing rather than reliance on any single element alone.1
But family history is not simply a checklist. It is a translation exercise. Family history increases suspicion, but it should be interpreted alongside the patient’s bleeding phenotype, laboratory pattern, testing conditions, and prior hemostatic challenges.
Families do not always say: we have von Willebrand disease.
They may say:
- the women in our family have terrible periods
- everyone gets nosebleeds
- we bruise easily
- my mother needed a hysterectomy
- my sister bled after childbirth
- my uncle always bled after dental work
- my child bled after tonsillectomy
- no one ever called it anything
Family history is often described narratively before it is recognized medically. The clinician must know how to hear these sentences as possible hemostatic history.
The family that thinks bleeding is normal
Families normalize what they share. This is human. A child learns what is ordinary from the people around them.
If a mother has heavy periods, a daughter may assume heavy periods are expected. If siblings get nosebleeds, nosebleeds become family trivia. If bruises are common, bruising becomes personality. If postpartum hemorrhage happened to several relatives, childbirth may simply be remembered as dangerous.
The problem is not that families are careless. The problem is that inherited disease can disguise itself as family normal.
Shared symptoms can obscure shared pathology.
VWD may be hidden precisely because it is shared. This is especially important for heavy menstrual bleeding, which may be normalized across generations before it is recognized as a bleeding phenotype.2
Diagnosis changes the past
A diagnosis does not only explain the present. It revises the past.
After VWD is diagnosed, old events may take on new meaning:
- childhood nosebleeds
- emergency dental visits
- years of iron deficiency
- missed school during menses
- transfusion after delivery
- unexplained surgical bleeding
- an aunt who “almost died” in childbirth
- a grandmother who had a hysterectomy young
- a relative who was “always a bleeder”
These events may have been disconnected. Diagnosis connects them. It creates a pattern where memory had only fragments.
Diagnosis does not change what happened. It changes what it means.
This can be validating. It can also be unsettling.
Recognition and relief
For some families, diagnosis brings relief.
The bleeding was real. It was not weakness. It was not exaggeration. It was not poor pain tolerance. It was not bad luck. It was not just “women’s problems.”
It had a name.
A diagnosis can transform family memory from confusion into recognition. A parent may say: I wish we had known. A patient may say: That explains everything.
Recognition can be healing because it restores legitimacy to experiences that were previously minimized.
Recognition and grief
Recognition can also bring grief.
If VWD explains the past, it may also reveal missed opportunities: years of iron deficiency, avoidable postpartum bleeding, unnecessary transfusion, delayed treatment, repeated dismissal, or a child’s surgery done without preparation.
Clarity can arrive too late to prevent harm.
A parent may feel sorrow that they did not recognize the pattern earlier. A patient may feel anger that no one asked. A family may feel that medicine arrived late.
Diagnosis can bring relief and regret at the same time.
Both responses are reasonable.
The shadow of blame
Inheritance can easily become blame.
A parent may wonder:
- Did I give this to my child?
- Should I have known?
- Did my side of the family cause this?
- Should I have been tested before pregnancy?
- Did we miss signs?
This emotional logic is powerful. It is also dangerous. Inherited conditions are often interpreted through moral language, even when they are biological.
Genes are transmitted, not assigned.
Inheritance is not fault.
A parent does not cause VWD by loving a child into existence. The clinician’s language matters. “Passed down” can sound like blame. “Inherited” can sound more neutral. “Runs in families” can normalize without accusing.
The goal is to explain transmission without moralizing it.
The inherited body is not a guilty body
A family may need to hear this plainly:
No one is to blame for an inherited bleeding disorder.
You did not choose your genes. You did not choose your child’s genes. You did not fail because you did not recognize a disease that had never been named.
What matters now is recognition, planning, and care.
Responsibility begins with care, not causation.
This is not sentimentality. It is clinical communication. Blame interferes with testing, disclosure, family discussion, and care. Removing blame helps the family use the diagnosis.
Variable expression and family confusion
VWD can be confusing within families because relatives may not look equally affected.
One person bleeds heavily. Another has low VWF but few symptoms. One sibling needs treatment. Another does not. A parent has borderline levels. A child has clear disease. A grandparent remembers no bleeding at all.
This variability is especially common in type 1 VWD and low VWF states, where penetrance, modifiers, blood group, age, sex-specific exposures, hemostatic challenges, and other factors influence phenotype.3
This can create family doubt:
- If my father has it but never bleeds, why do I bleed?
- If my sister’s tests are normal, why are mine abnormal?
- If my mother had heavy periods, why was she never diagnosed?
Shared inheritance does not produce uniform experience.
Inheritance is real. Expression is variable.
Both truths matter.
Autosomal does not mean identical
VWD is often autosomal. That means males and females can inherit the condition.
But equal inheritance does not mean equal experience.
People who menstruate, become pregnant, give birth, or undergo gynecologic procedures may encounter more frequent or more revealing hemostatic challenges. This is one reason VWD may become more clinically visible in females despite autosomal inheritance.4
The gene may be shared.
The life course is not.
Equal transmission does not produce equal exposure. A family may therefore see the disease more clearly in daughters, sisters, mothers, or aunts. That does not mean others are unaffected. It means exposure reveals risk.
When a child’s diagnosis reveals a parent
Sometimes a child is the first person diagnosed. Then the parent is tested.
Diagnosis can invert the direction of recognition.
The parent may learn that their own bleeding was not normal. This can be emotionally complex. The parent may feel validated. They may also feel guilt. They may think: I should have known. I gave this to my child. I dismissed their symptoms because mine were the same.
This is a difficult moment. It should be handled gently.
The child’s diagnosis does not indict the parent.
It illuminates the family.
When a parent’s diagnosis protects a child
The reverse can also happen. A parent’s diagnosis may protect a child before bleeding occurs.
A newborn may avoid unnecessary procedures without planning. A child scheduled for tonsillectomy may be evaluated first. A teenager with heavy menstrual bleeding may be recognized sooner. A family may have tranexamic acid, desmopressin testing, or VWF replacement plans available before crisis.
This is the practical value of family history. It turns inherited risk into anticipatory care.
Knowledge converts inheritance into prevention.
The purpose of knowing is not fear.
It is preparation.
The ethics of telling relatives
Inherited disease creates responsibility beyond the individual.
If one person is diagnosed, should relatives be told? Which relatives? How much should be said? Who should say it? What if the family is estranged? What if the diagnosis is uncertain? What if relatives do not want to know?
VWD is often manageable, but the information can still matter. It may affect surgery, childbirth, dental work, pregnancy, postpartum care, anticoagulation, and evaluation of heavy menstrual bleeding.
Information benefits families, but disclosure belongs to individuals.
Patients may need guidance on how to communicate. The clinician can help by providing clear language:
This is an inherited bleeding disorder or bleeding tendency. Relatives with heavy bleeding, planned surgery, childbirth history, or significant nosebleeds may benefit from discussing testing with their clinician.
Disclosure should be encouraged as care, not imposed as accusation.
Testing relatives
Family testing is not always straightforward.
The value and interpretation of family testing differ by subtype. Testing is clearer for type 3 VWD, type 2N VWD, and some type 2 variants. It is more uncertain in type 1 VWD and low VWF borderlands.
Inheritance counseling is subtype-specific: type 1 VWD often shows autosomal dominant inheritance with variable penetrance; type 3 VWD and type 2N VWD are typically recessive; and apparent type 2B VWD may require distinction from platelet-type VWD.5
A relative with no bleeding history and borderline VWF may not need the same label as the proband. Testing should be interpreted with bleeding history, age, prior hemostatic challenges, and clinical context.
Testing is most useful when it changes practical planning:
- surgery
- dental extraction
- childbirth
- heavy menstrual bleeding evaluation
- anticoagulation decisions
- emergency care
- family planning in severe or recessive forms
The goal is risk stratification, not universal labeling.
The goal is not to create a family of patients.
The goal is to identify who needs hemostatic planning.
Family history as a living document
Family history should not be collected once and abandoned.
It changes. A sister develops heavy menstrual bleeding. A cousin bleeds after dental extraction. A parent has surgery. A relative has postpartum hemorrhage. A child reaches adolescence. A genetic result becomes available. A diagnosis is revised.
Family history evolves as new hemostatic challenges occur. The family map changes as life creates new evidence.
In VWD, a family history should be a living document, not a static checkbox.
When families resist the diagnosis
Not every family welcomes a genetic explanation.
Some may resist because they fear blame. Some worry about stigma. Some distrust medical labels. Some do not want children labeled. Some have normalized bleeding for generations. Some fear insurance or employment consequences. Some simply do not want to revisit painful events.
Resistance is not ignorance. It may be protective. It may also reflect prior experience of harm from labeling.
The clinician’s task is not to force identity. It is to explain the practical stakes:
- what situations require planning
- what relatives may be at risk
- what symptoms should prompt evaluation
- what can be done to prevent harm
Inherited risk and patient autonomy
Family information belongs partly to the patient and partly to the family. This creates tension.
A patient may not want to tell relatives. But relatives may benefit from knowing. A clinician may feel responsible to the wider family. But confidentiality remains central.
Most VWD situations can be handled through counseling, education, and patient-mediated disclosure. The patient can be supported with written language, family letters, and clear explanation.
Most ethical solutions rely on supported disclosure, not forced communication.
The ethical stance is to respect the patient’s autonomy, recognize the family relevance, and make communication easier.
The family letter
Sometimes families need a simple written explanation.
A possible family letter might say:
I was diagnosed with von Willebrand disease, an inherited bleeding disorder that can cause heavy menstrual bleeding, nosebleeds, bruising, dental bleeding, surgical bleeding, or postpartum bleeding. Because it can run in families, relatives who have bleeding symptoms or who are planning surgery, dental extraction, pregnancy, or childbirth may want to discuss testing with their clinician or a hematologist.
This kind of language matters. It reduces the emotional charge, makes the information practical, avoids blame, and invites awareness.
The child who does not want to be different
Children and adolescents may experience inherited diagnosis as difference.
They may not want to be the child with a bleeding disorder. They may not want restrictions. They may not want teachers to know. They may not want parents to worry. They may not want siblings tested because of them. They may feel responsible for family anxiety.
The goal is not to make the child feel fragile.
It is to make them competent.
A child with VWD can learn:
- when to tell an adult
- what bleeding matters
- what medicine helps
- why dental and surgical planning matters
- how to participate safely
- how to explain the condition simply
Competence is more protective than protection.
Knowledge should increase freedom, not shrink it.
The sibling question
Siblings create another emotional layer.
One child is diagnosed. Another is tested. One has low levels. Another does not. One needs precautions. Another feels ignored. One feels guilty for being healthy. One feels resentful for being watched.
Genetic differences can become emotional differences within families.
Families may need help distributing attention fairly. The clinician’s role may include explaining that different results do not mean different worth.
They mean different hemostatic risk.
The reproductive meaning of inheritance
For some patients, VWD becomes most emotionally charged when thinking about children.
Will my child have this? Will pregnancy be safe? Will delivery be dangerous? Should my partner be tested? What if we both carry severe variants? Could a child have type 3 VWD?
Reproductive decisions transform inheritance into future responsibility.
These questions are especially important in type 3 VWD, type 2N VWD, consanguinity, or families with severe disease. Genetic counseling may help clarify risk, options, and uncertainty.6
But counseling should not be reduced to arithmetic. It should also make room for fear, hope, and responsibility.
Genetics without determinism
Genetic language can sound deterministic.
You have the variant. You will bleed. Your child will bleed.
But VWD rarely behaves with that simplicity, especially in type 1 VWD and low VWF. A genetic tendency may produce different bleeding patterns in different people. The same family may contain severe bleeding, mild bleeding, and almost no bleeding.
The phenotype depends on VWF level, subtype, modifiers, sex-specific exposures, age, procedures, pregnancy, comorbidities, and chance.
Genetic information informs probability, not destiny.
Genetics gives information.
It does not remove uncertainty.
When the family history is absent
Some patients with VWD have no clear family history.
This can happen for many reasons: family members may not have been tested, bleeding may have been normalized, the patient may be adopted, relatives may be unavailable, inheritance may be recessive, penetrance may be incomplete, or the patient may be the first recognized case.
Absence of history may reflect absence of recognition.
Absence of family history does not exclude VWD. It means the family story may not yet have been medically translated.
When family history misleads
Family history can also mislead.
A relative may have bled because of anticoagulation. Heavy periods may have been caused by fibroids. Postpartum hemorrhage may have been obstetric. A relative may have liver disease, platelet dysfunction, or another bleeding disorder. A family may report “hemophilia” when the actual disorder is VWD.
Family narratives require clinical interpretation.
The clinician should listen carefully but not accept every family label uncritically.
Family history is a clue.
It is not a diagnosis.
The inherited body and self-understanding
An inherited diagnosis changes how a person understands their body.
The body is no longer only individual. It becomes connected to parents, children, siblings, ancestors, and future generations.
The body becomes a link across generations.
This can feel grounding. It can also feel heavy.
A patient may think:
- my body carries my family’s pattern
- my child’s body may carry mine
- my bleeding is not only mine
This is one of the deep humanities dimensions of VWD.
The disease is biological, but its meaning is relational.
What clinicians can do well
Clinicians can help families by:
- asking family history in concrete bleeding terms
- avoiding blame language
- explaining variable expression
- clarifying inheritance pattern by subtype
- distinguishing diagnosis from risk
- providing written information for relatives
- encouraging evaluation of symptomatic relatives
- supporting adolescents without making them feel fragile
- recommending genetic counseling when appropriate
- documenting practical implications for surgery, childbirth, dental work, and emergency care
- revisiting family history over time
Language shapes whether inheritance feels like burden or preparation.
Good family care turns inheritance into preparation rather than guilt.
Clinical synthesis
VWD is inherited biologically, but it is lived relationally.
Family history may reveal patterns of heavy menstrual bleeding, nosebleeds, bruising, dental bleeding, postpartum hemorrhage, hysterectomy, surgical bleeding, or anemia that were never previously named. Diagnosis can bring relief, recognition, grief, guilt, and responsibility.
Inheritance should be explained without blame. Variable expression should be expected. Family testing should be guided by subtype, bleeding history, clinical context, and practical implications.
The purpose of recognizing inheritance is not to create anxiety. It is to make hidden risk visible early enough to prevent harm.
VWD is not only a disorder of the individual body. It is a disorder that often teaches a family to read its own history differently.
In VWD, inheritance is not only a mechanism.
It is a relationship.
Reflect & Apply Case
A 13-year-old girl is diagnosed with type 1 VWD after heavy menstrual bleeding, recurrent epistaxis, and low ferritin.
Her mother says:
“I had terrible periods too. My mother had a hysterectomy at 38. I thought this was just our family.”
The mother becomes tearful and asks:
“Did I give this to her?”
Questions for reflection:
- How can the clinician explain inheritance without blame?
- What parts of the family history are clinically relevant?
- Why might heavy menstrual bleeding have been normalized across generations?
- Which relatives might benefit from evaluation?
- How should variable expression be explained?
- What practical information should the family receive for future procedures or pregnancies?
- How can the diagnosis be framed as recognition rather than accusation?
This case illustrates the central lesson:
inheritance is not fault.
It is information that can protect the next person.
Evidence anchor: why inheritance changes family meaning in VWD
Summary derived from diagnostic guidelines, patient-experience literature, genetic reviews, low-VWF literature, and management guidance. The evidence consistently shows that inheritance in VWD is not only a genetic fact; it affects recognition, testing, communication, and family planning.
| Evidence stream | What it shows | Why it matters | Main limitation |
|---|---|---|---|
| Family history in diagnosis | VWD diagnosis requires integration of bleeding phenotype, family history, laboratory results, testing conditions, and prior hemostatic challenges.7 | Family history can reveal inherited bleeding patterns, but it should not replace phenotype and laboratory interpretation. | Family stories may be incomplete, normalized, inaccurate, or shaped by prior medical labels. |
| Family normalization | Heavy menstrual bleeding, nosebleeds, bruising, postpartum hemorrhage, hysterectomy, and iron deficiency may be normalized across generations before being recognized as hemostatic evidence.8 | What families call “normal” may be inherited bleeding risk. | Normalization can obscure disease, but shared symptoms do not prove VWD. |
| Variable expression | Type 1 VWD and low VWF states often show variable bleeding expression within families, influenced by VWF level, blood group, age, sex-specific exposures, hemostatic challenges, and other modifiers.9 | Shared inheritance does not produce uniform experience. One relative may bleed heavily while another has few symptoms. | Variable expression can make families doubt the diagnosis or overgeneralize risk. |
| Sex-specific exposure | VWD is inherited in all sexes, but menstruation, pregnancy, childbirth, and gynecologic procedures make bleeding risk more visible in many females.10 | Equal inheritance does not mean equal exposure or equal recognition. | Male relatives may still carry clinically relevant risk for procedures, trauma, or later-life bleeding. |
| Subtype-specific inheritance and testing | Type 1 often shows autosomal dominant inheritance with variable penetrance; type 3 and type 2N are typically recessive; apparent type 2B may require distinction from platelet-type VWD. Genetic counseling may be useful in severe, recessive, or diagnostically complex cases.11 | Family testing should be guided by subtype, phenotype, and practical implications, not applied indiscriminately. | Genetic testing may not resolve uncertainty in type 1 VWD or low VWF borderlands. |
| Management implications for relatives | A family diagnosis may change planning for surgery, dental extraction, pregnancy, delivery, postpartum care, heavy menstrual bleeding, anticoagulation, or emergency bleeding.12 | The purpose of inheritance recognition is prevention and preparation, not blame. | Treatment decisions remain individualized by subtype, bleeding phenotype, procedure type, and response to therapy. |
Interpretive note: These evidence streams support the essay’s central claim: inheritance in VWD is both biological and relational. A family history can make hidden bleeding visible, but it can also create guilt, uncertainty, and responsibility. The task is to translate inheritance into preparation without turning it into blame.
Family guidance: explaining inheritance without blame
Based on diagnostic guidance, genetic reviews, patient-experience literature, and management recommendations.
Ask family history in concrete bleeding terms
Do not ask only, “Does anyone have VWD?” Ask about:
- heavy menstrual bleeding
- iron deficiency or anemia
- postpartum hemorrhage
- transfusion after childbirth or surgery
- hysterectomy for heavy bleeding
- recurrent epistaxis
- easy bruising
- gum bleeding
- dental extraction bleeding
- tonsillectomy or surgical bleeding
- “bad bleeders” in the family
- known VWD, hemophilia, platelet disorders, or unexplained bleeding
Explain inheritance without moralizing
Useful language:
- “This runs in families, but no one caused it.”
- “Genes are transmitted, not assigned.”
- “Inheritance is not fault.”
- “The purpose of knowing is preparation, not blame.”
- “Different relatives can have different bleeding patterns.”
- “A parent’s diagnosis can protect a child before a bleeding challenge occurs.”
- “A child’s diagnosis can help a parent understand their own history.”
Decide who may benefit from evaluation
Consider evaluation for relatives who have:
- heavy menstrual bleeding
- recurrent nosebleeds or easy bruising
- iron deficiency or anemia
- prolonged bleeding after dental extraction or surgery
- postpartum hemorrhage
- planned surgery, dental extraction, pregnancy, childbirth, or anticoagulation
- a close relative with definite VWD, especially type 2, type 3, severe type 1, or unclear subtype
- reproductive concerns in families with type 3 VWD, type 2N VWD, consanguinity, or severe disease
Avoid common pitfalls
- assuming shared bleeding is normal because it is common in the family
- assuming lack of family history excludes VWD
- assuming all relatives need the same diagnostic label
- using “passed down” in a way that sounds accusatory
- treating genetic information as destiny
- testing relatives without explaining how results will change planning
- forgetting male relatives because menstrual bleeding is the most visible family symptom
- treating family history as a one-time checkbox rather than a living document
A possible family message
I was diagnosed with von Willebrand disease, an inherited bleeding disorder that can cause heavy menstrual bleeding, nosebleeds, bruising, dental bleeding, surgical bleeding, or postpartum bleeding. Because it can run in families, relatives who have bleeding symptoms or who are planning surgery, dental extraction, pregnancy, or childbirth may want to discuss testing with their clinician or a hematologist.
Practical takeaway: Family history is not only a pedigree. It is a pattern of bleeding, memory, and opportunity. Good counseling turns inherited risk into preparation rather than guilt.
Reflect & Apply Case
A 13-year-old girl is diagnosed with type 1 VWD after heavy menstrual bleeding, recurrent epistaxis, and low ferritin.
Her mother says:
“I had terrible periods too. My mother had a hysterectomy at 38. I thought this was just our family.”
The mother becomes tearful and asks:
“Did I give this to her?”
Questions for reflection:
- How can the clinician explain inheritance without blame?
- What parts of the family history are clinically relevant?
- Why might heavy menstrual bleeding have been normalized across generations?
- Which relatives might benefit from evaluation?
- How should variable expression be explained?
- What practical information should the family receive for future procedures or pregnancies?
- How can the diagnosis be framed as recognition rather than accusation?
This case illustrates the central lesson:
inheritance is not fault.
It is information that can protect the next person.
Test your thinking
A short quiz on family history, inheritance, and responsibility in VWD.