CASE OF THE WEEK
When a disease stops behaving like itself

Sort the following into categories:
Richter transformation
Infection or abscess
Inflammatory process
Metastatic disease
Pancreatic or biliary malignancy
Indolent progression
CLL-related processes
Non-CLL malignancy
Non-malignant
Match each finding to its interpretation:
Elevated LDH
Mild anemia
Stable WBC
Nonspecific (chronic disease, marrow involvement, or prior therapy)
Does not exclude transformation; may reflect shift away from circulating disease
High cell turnover / aggressive process
Correct!
Sorry, Incorrect.
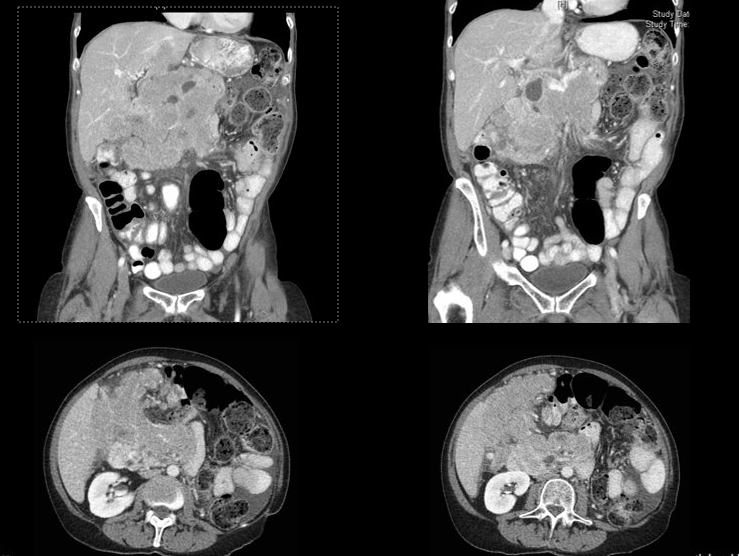
Imaging
CT scan shows:
- Large heterogeneous right upper quadrant mass
- No widespread bulky lymphadenopathy
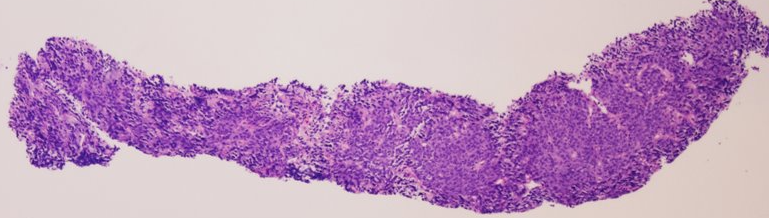
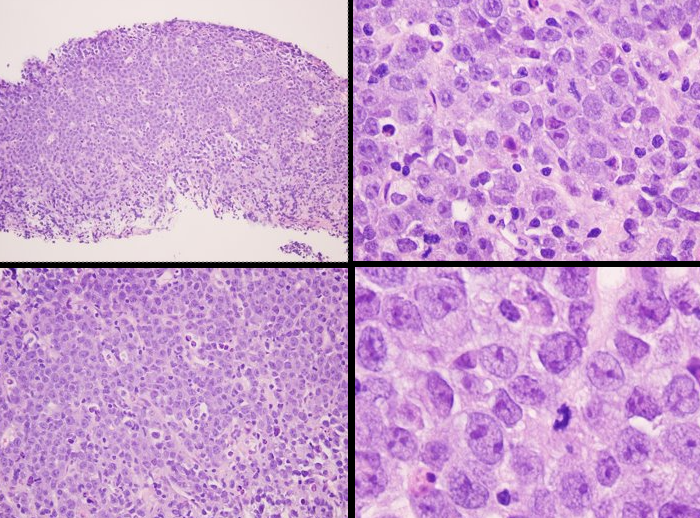
Biopsy (initial findings)
- Large atypical cells
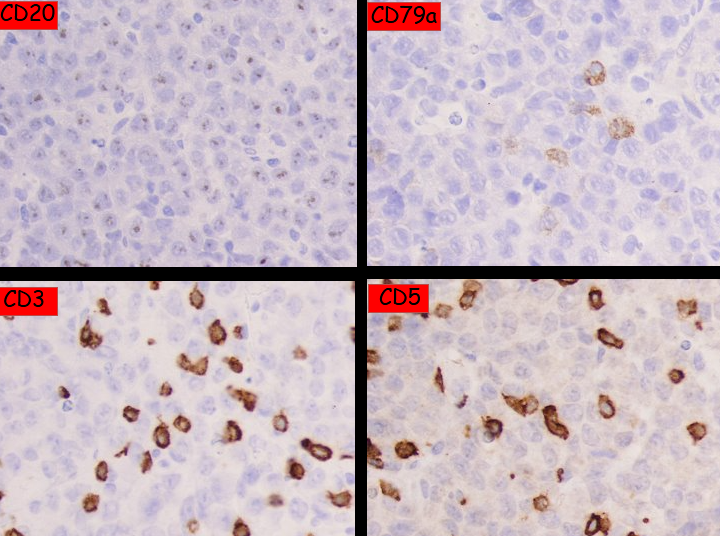
- Negative for CD20
- Negative for CD3
CT-guided Core Needle Biopsy of Abdominal Mass
Sort the following features:
Focal mass
Lymphocytosis
Stable CBC
Rapid growth
High LDH
Transformation:
CLL progression: